A small but select group of trainees met at the North Middlesex Hospital for a day featuring: palliative and end of life care; TB; SLT perspectives on aspiration; and home NIV. Many thanks to Dr Stefan Lozewicz for co-ordinating the day.

Palliative Care
Dr Vinnie Nambisan, Consultant in Palliative Care, started the day with a topical subject, palliative and end of life care. Many of us heard discussion of the BMA’s latest report (End-of-life care and physician-assisted dying) on Radio 4 as we got up or were travelling to North Mid. The three overarching themes of the report are:
- The need to ensure the provision of consistently high-quality end-of-life care
- The need for ongoing education, training and support for doctors
- The central role of families and those close to the patient
We considered the importance of generalist palliative care, which we should all have some knowledge of, and what specialist palliative care services provide in addition.
- All palliative care services will accept referrals for care in the last few weeks of life.
- Hospice admission may be reserved for those with a high level of need, rather than solely patient choice.
- Community palliative care is usually not able to keep people on caseloads if they have no current needs.
- Palliative care specialists are experts in end of life care, advance care planning, palliative rehab, respite, symptom control, and psychological support.
The GMC 2010 definition of patients ‘approaching the end of life’ are those likely to die within the next 12 months. This includes patients whose death is imminent (expected within a few hours or days) and those with:
- advanced, progressive, incurable conditions
- general frailty and co-existing conditions that mean they are expected to die within 12 months
- existing conditions if they are at risk of dying from a sudden acute crisis in their condition
- life-threatening acute conditions caused by sudden catastrophic events
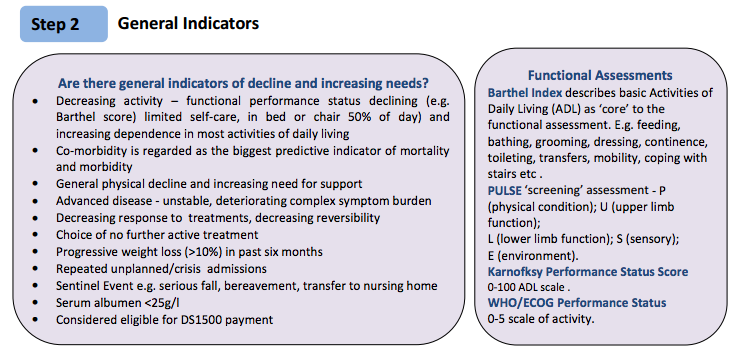
In order to provide good end of life care we must recognise that a person is dying. The Gold Standards Framework (GSF) provides some guidance but is predominantly community-based. It provides a structured approach, using the surprise question, some general indicators, and some disease specific indicators.
We have all seen the dying trajectories for cancer, organ failure and frailty/dementia, discussed by Murray et al. Even these patterns are not very helpful as trajectories don’t fit to individuals in reality so there is significant uncertainty. Signs that a person is dying in days/hrs include: diagnosis, change in condition, drowsiness, unconsciousness, decreased oral intake, decreased urine output, reduced mobility, fatigue, laboured breathing, and investigation results. A mix of clinical and non-clinical factors, and multidisciplinary team input is recommended.
If it is clear someone is dying, how do you then tell them? We discussed situations in which it may be appropriate or inappropriate to start such as discussion. It is paramount to check that the person actually wants to know (asking ‘how long have I got’ does not always refer to life/death), and to establish what they already know. It was recommended we talk in categories rather than specifics – years, months, long wks, short wks, days, hours. Acknowledge uncertainty is also important eg “it’s not possible to be accurate and we can’t know for certain but…”
The Leadership Alliance for the Care of Dying People has published a number of reports, including “One chance to get it right”. The alliance highlight five priorities for care that should be the touchstone for every point of care for those in the last days and hours of life and their families – from frontline health and care staff to commissioners and regulators.
- The possibility that a person may die within the coming days and hours is recognised and communicated clearly, decisions about care are made in accordance with the person’s needs and wishes, and these are reviewed and revised regularly.
- Sensitive communication takes place between staff and the person who is dying and those important to them.
- The dying person, and those identified as important to them, are involved in decisions about treatment and care.
- The people important to the dying person are listened to and their needs are respected.
- Care is tailored to the individual and delivered with compassion – with an individual care plan in place
The last of these priorities is related to the fact that the LCP was withdrawn in July 2014, having become overly politicised. Prof Neuberger lamented that it had become a tainted brand, and was unsalvageable. There were of course problems in the way that some people applied the, but the LCP itself was a very helpful framework for many. We reviewed some specific points in the new guidance – we should not make changes to anything without discussion with relatives/NOK unless it is absolutely necessary. Any major decisions should be made in normal working hours. In place of the LCP Trusts now have individualised care plans. It is important to become familiar with the care plan in the hospital in which you work.
For symptom control, flow charts are helpful and prompt anticipatory prescribing. No patient should have to wait for end-of-life medications. Breathlessness is a common symptom for Respiratory patients and can be alleviated using both pharmacological and non-pharmacological strategies.
- Lok, Chan Wing. “Management of Breathlessness in Patients With Advanced Cancer A Narrative Review.” American Journal of Hospice and Palliative Medicine (2014): 1049909114554796.
Dr Nambisan also recommended the Scottish palliative care guidelines, which are clear and practical. Another important aspect of anticipatory prescribing is ensuring that patients who go home have access to medication. There is specific paperwork that is essential to authorise administration of medicines outside the hospital including an order for a community nurse to administer medications. Unfortunately there is no standardised documentation so there are different forms in every borough! When prescribing, be as clear as possible: set limits on doses/increases, and be open to review/change.
We moved on to discuss DNACPR, and the gap between the clarity of guidance and the complex nuances of real life situations. We touched on important learning from the Tracey case (2012), in which it was ruled that human rights had been breached.We also discussed the case of Carl Winspear (2015), a man with cerebral palsy, who lacked capacity to make decisions about his DNACPR status. A DNACPR was made for him at 3am by an on call doctor in hospital, without consultation with his mother. It was then cancelled in the morning. The failure to consult his mother was deemed to have breached the Mental Capacity Act, and Carl’s Article 8 human rights. Dr Nambisan feels that second opinions are under-utilised regarding DNACPR decisions and are a valuable way of continuing to keep lines of communication open when there is conflict between the view of healthcare professionals and family.
Tuberculosis
Dr Sam Perkins of the South London Health Protection Team gave us an update on TB epidemiology, using WHO data. There are 1.5million deaths/yr globally, 140,000 of whom are children. There are an estimated 9.6 million cases, only 2/3 of which are diagnosed. There are an estimated 480,000 MDR-TB cases globally, only 1/4 of which are detected/reported. 105 countries now have reported XDR-TB.
Public Health England publishes data on TB in England. There are 12/100,000 cases in England, but in London this is 30/100,000. The well-known North London isoniazid resistant outbreak has been linked with drug taking, prison population and used car dealers!? Within London Brent and Newham are TB hotspots, with rates approaching 100/100,000. The PHE Annual Review for London has individual borough data – including high rates in Enfield and Haringey. Health inequalities are a key part of TB care – 1 in 10 patients also have drug or alcohol dependency, homelessness or imprisonment. 83% are non-UK born, 58% male, 44% unemployed.
We were given an insight into the work of Public Health workers during an outbreak. A ‘TB incident’ is defined as sputum smear positive pulmonary TB and ‘significant exposure’ – in London the guidance is >8hrs/wk in a congregational setting (e.g. educational, workplace, healthcare, detention, social and other venues).
We discussed a case to further explore the role of public health doctors. We considered a patient with MDR-TB who is not compliant with DOT. We discussed attempting persuasion for admission, linking with key workers, and with Find and Treat, the use of incentives (may need to negotiate and be pragmatic!). We then considered what is involved in a part 2A order under the Public Health Act (HPA Regulations 2010). Dr Perkins affirmed that a Part 2A order is a blunt tool and is not an easy solution to this problem – it takes time to get necessary paperwork, and each order only lasts 28days. The order can be placed on people, premises, or things! There are penalties of up to £20,000 if a patient breaches the order (but who can pay this anyway!?). It is important to remember that a patient cannot be forced to accept treatment, even if quarantined. All other avenues should have been pursued before considering a Part 2A. If it is felt to be necessary, an application must be made to a magistrate by the Proper Officer of the Local Authority (which can be tricky if the patient is homeless). The application must specify where the patent will be detained (a Trust must agree, and there is a need to consider what constitutes reasonable force in advance, with agreements in place with Police if the patient absconds). Long-term planning/discharge planning is essential from the beginning. The DoH produces a guide on how to go about applying for Part 2A order.
NICE guidelines were updated Jan 2016. The upper age limit for offering tests and treatment for latent TB is now 65yrs. Another change is the definition of a positive Mantoux: any patient regardless of BCG history with skin induration >5mm (this will lead to an increase in referrals). It is recommended that NAATs are requested for MTB on primary specimens if there are risk factors for MDRTB. On the updated guidance there are new criteria for ‘at risk’ and new guidance on hepatotoxicity and re-establishing treatment after interruptions. The Collaborative TB Strategy 2015-2020 sets out ten priority areas. It includes systematically implementing new entrant LTBI screening (in primary care).

They have even made an infographic!
Fit to fly? Who needs oxygen on commercial flights?
xxxx Commercial air planes are maintained at a pressure equivalent of 8000ft altitude. In official figures, almost 10% of in-flight emergencies are respiratory, but it may be more than this. The risks of air travel include gas expansion (Boyle’s law – trapped gas expands by around 30%, increase RV and reduce respiratory reserve, risk of barotrauma).
- Malhotra, M. S., and H. C. Wright. “The effects of a raised intrapulmonary pressure on the lungs of fresh unchilled cadavers.” The Journal of pathology and bacteriology 82.1 (1961): 198-202.
There are also other rarer complications:
- Zaugg, Michael, et al. “Fatal air embolism in an airplane passenger with a giant intrapulmonary bronchogenic cyst.” American journal of respiratory and critical care medicine 157.5 (1998): 1686-1689.
A number of bodies produce guidelines for air travel: the Aerospace Medical Association, and the UK CAA. A common question is when can someone fly after resolution of a pneumothorax – 2wks. It is also safe to travel with a Heimlich valve.
Hypoxia is the major concern for air travel. The reduced atmospheric pressure equates to 15% of that at sea level. In a healthy person, at up to 8000ft no physiological adaptation is needed to maintain a PaO2 > 8Kpa. If someone has a baseline PaO2 of 9kPa a patient will desaturate to sats of 65%. If acidotic this is even worse. Patients may hyperventilate with normal sats, or be very hypoxic but asymptomatic (but at risk). Indirect methods of assessing whether someone is fit to fly do not work. Prediction equations do not take individual responses into account and have been shown to be unreliable. The gold standard for assessment is a hypobaric chamber. This is not available outside the military as it is prohibitively expensive. Alternatives are:
- Hypoxic inhalation test – FiO2 15% (mixed with nitrogen in bag, in body box, or 40% venturi mask driven with nitrogen). But £300 for cylinder of nitrogen = 3 tests. Pricey.
- Hypoxicator – oxygen concentrator in reverse. Mains-powered hypoxic gas generation: a cost-effective and safe methods evaluate patients at risk from hypoxia during air travel. Validated as equivalent of going on plane or hypobaric chamber. And cheaper!
During a hypoxic challenge test, if sats are maintained >90% after 20min then the patient is fit to fly. If sats 85-90% a blood gas is taken after 20minutes —> if PaO2 >6.6kPa OK, if <6.6kPa add Oxygen (max 4L) then after another 20min PaO2 >6.6kPa safe to fly. If can’t keep above 6.6kPa unfit to fly.
Interestingly pCO2 is not part of the current guidelines. We reviewed a case in which this was concerning! Hypoxic challenges are done even within 6wks of infection, since people choose to fly at this interval and so should be assessed if necessary. Obviously, no patient should fly with active TB. Following a pleural effusion it is fine to fly immediately IF NO AIR – confirm with CT? We discussed the rules regarding NIV and CPAP machines. Patients can take NIV machines on to planes, but this is at the discretion of the airline, and can’t be used for take off or landing. Patients have to have someone to sit with them and bag them for the first and last hour if they are NIV dependant! Oxygen is also at the discretion of the airline. Most provide oxygen, but only specific devices which are FAA approved. And importantly, if an airline provides in-flight oxygen, they do not provide oxygen for any changes or stopovers, so patients need to liaise with the airport in addition to the airline.
Speech and Language Therapy take on aspiration pneumonia
Sarah Hughes started by reviewing the anatomy and physiology of swallowing. We were reminded of the close proximity of the trachea and oesophagus, and of the problems of an upright stature when in comes to preventing aspiration. We ran through the stages of swallowing: the pre-oral stage; oral stage (negative intra-oral pressure); and the pharyngeal stage (breathing must cease to swallow safely). Respiration is inhibited for 0.6-2.0 seconds during swallowing. We were sad to hear that as we age, our swallow ages too. From the very young age of 40 onwards these changes are apparent!
There are several breath swallow patterns, as characterised by Matsuo and Palmer 2009.
- exhale-swallow-exhale & inhale-swallow-exhale are OK
- exhale-swallow-inhale & inhale-swallow-inhale are problematic
Red flags for aspiration risk include: recurrent chest infections, weight loss, reduced mobility, reliance on others for feeding, and poor dentition. Unilateral chest/CXR changes are said to be a red flag, but in practice both L and R midzone/base pneumonias are seen. In addition, we were advised to note candida/oropharyngeal flora/colonisation and dehydration as these are also risks. A number of factors have been associated with aspiration pneumonia. Dysphagia was found to be necessary but not sufficient in one study, with other factors such as dependency for feeding, poor dentition, tube feeding, polypharmacy and comorbidities.
- Langmore, Susan E., et al. “Predictors of aspiration pneumonia: how important is dysphagia?.” Dysphagia 13.2 (1998): 69-81.
It’s important to investigate, but also to be mindful of the limitations of tests. Video fluoroscopy is not always reliable. It is merely a snapshot in time, and therefore cannot quantify risk, only inform the overall clinical picture. There is no way to tell conclusively that a pneumonia is definitely an aspiration pneumonia.
The Parkinson’s Society has some very helpful guidelines on converting oral PD medications to patches/iv preparations, which is essential if there are any delays to NG insertion. There is no excuse for causing deterioration due to a gap in medications. NG tubes should be a short term measure. But how long is short term?
Swallowing assessment in patients with severe COPD was said to be particularly challenging. These patients often have chronic, but fluctuating dysphagia. Neuropsychological impairments in attention, memory, and abstract thought processes may be particularly relevant in hypoxaemic patients. Interestingly, lung volume also affects pharyngeal swallow physiology. In COPD patients may have premature resumption of breathing, increasing the risk of aspiration. In addition, many have reflux, which has been linked to exacerbations.
- Gross, Roxann Diez, et al. “Lung volume effects on pharyngeal swallowing physiology.” Journal of Applied Physiology 95.6 (2003): 2211-2217.
- Terada, Kunihiko, et al. “Abnormal swallowing reflex and COPD exacerbations.” CHEST Journal 137.2 (2010): 326-332.
We finished the session with some cases, which underlined the importance of using all available evidence to make a risk assessment. Conversations about future risk and prognosis were also highlighted as important as part of the management of the patient and their families.
Difficult TB
Dr Stefan Lozewicz took us through some cases, in which we were advised to ask ‘is this TB?’ and ‘how should I manage this case?’ We reviewed the risk factors for TB: ethnic group, deprivation, social factors, contact, HIV. We also recalled the areas of the world from which there is an excess of cases in London: India, Pakistan, Somalia.
We all knew that 8hrs exposure to someone with smear +ve pulmonary TB is generally felt to be necessary for a significant risk of transmission. But few of us knew that this figure was based on flight data! An 8hr flight within 2rows of an index smear +ve pTB person outs you at significant risk of transmission. However this does not account for cumulative exposure, such as that of healthcare professionals.
From either induced sputum or bronch a 40% culture rate can be expected. Culture positivity rate on EBUS is just under 50%. We considered some cases and debated whether it was justified to start treatment on the basis of a CXR and history. There was debate in the room as to whether a CT +/- EBUS should be requested.
We were reminded of what LN TB looks like and were encouraged to aspirate peripheral nodes for analysis (you can DOPS that). We discussed the fact that even if smear -ve it would be reasonable to start treatment and review in the case of typical presentation. We then touched on paraspinal and cerebral TB and their complications. Cerebral TB has a high mortality rate. 50% are smear positive. 50-90% are culture positive in TB meningitis. The LP fluid is typically lymphocytic. It is wise to request PCR as this has a higher sensitivity than smear, and is faster than culture. However, sensitivity is less than a routine culture (on average) from any site. We got worried about hydrocephalus and agreed that there should be a low threshold for a CT if there was any suspicion of this complication.
We revised the differential for a lymphocytic meningitis – syphilis, Lyme disease, HIV, listeria, cryptococcus, autoimmune, sarcoidosis, partially treated bacterial meningitis.
The PHE annual TB report includes a wealth of useful data. England 2014 data showed that 32.9% of all cases were not confirmed by any lab method (culture, microscopy, histology or PCR). 4% used PCR.
We covered a number of areas of TB treatment that make popular SCE questions. We were reminded that standard therapy is 2RHZE 4RH, and that Moxiflox trials have not been successful in reducing the length of treatment. In CNS TB the continuation phase is 10 months. In CNS and pericardial TB corticosteroids should be added to treatment. The dose is 4mg/kg/day Pred, reduced over 4-8/52. For pericarditis it is 1mg/kg for 2-3/52.
Knowledge of CSF penetration of drugs is key: Pyrazinamide, Isoniazid, and Moxifloxacin have good penetration. Rifampicin, Ethambutol, Streptomycin, and Ciprofloxacin have poor penetration.
In Isoniazid-resistance (which many trainees will be familiar with due to the London Isoniazid-resistant outbreak) the recommendation is 2RZE 7RE (up to 10 months for extensive disease)
Unfortunately, side effects are common on TB treatment. Quadruple therapy often leads to anorexia+ vomiting. If the patient has normal LFTs then simple advice is helpful: take tablets after meals, split the dose and/or use an antiemetic. If AST/ALT are 5x normal then stop therapy (RZH). If less, continue and monitor. When fall back to 2x normal can reintroduce E and H then R then Z (or may choose to omit Z).
If there is skin itching but no rash – give an antihistamine. If there is a rash the most likely culprit is pyrazinamide.
- Tan, W. C., et al. “Two years review of cutaneous adverse drug reaction from first line anti-tuberculous drugs.” Medical Journal of Malaysia 62.2 (2007): 143.
If there is a poor response to treatment a number of factors should be considered:
- Poor compliance – risk assessment includes drug/EtOH/homelessness. Also DNAs, -ve urine tests, poor clinical response. Use DOT if compliance is an issue – it can be administered at hospital, at home, at a hostel…. make it work.
- MDR-TB – Eastern Europe, previous treatment, contact with MDR-TB. Check the WHO report for more info.
- Poor absorption e.g. diarrhoea
- Diagnosis wrong/co-infection
- Paradoxical reactions (can occur in LN, pleural effusion, pull lesions, cerebral tuberculoma, hydrocephalus) – use steroids.
- Cancer vs TB.
Don’t forget http://www.tbdrugmonographs.co.uk – a brilliant resource supporting the monitoring and safe use of anti-TB drugs (authors include Dr Will Rickets and Dr Jess Potter!)
Home NIV
Dr Moonsie took us through a number of cases and asked us to think about indications for and access to home NIV. He encouraged us to take into account the evidence, and to focus on selecting those patients who benefit.
He took us through the pattern for a normal sleep cycle: wakefulness —>NREM sleep —> REM sleep. Nocturnal hypoventilation occurs when there is an imbalance between load and capacity. This generally occurs in REM sleep. REM hypoventilation leads to arousals/awakening. If untreated e.g. with CPAP then bicarbonate rises, and eventually there is daytime respiratory failure. There is a lack of evidence for home NIV for eg COPD, particularly a lack of RCTs. Most evidence is from observational data: cohorts and case-control studies. There are no BTS guidelines, and great variation in practice within and between countries. The benefits of home NIV are symptomatic i.e. daytime performance, dyspnoea, QoL. There is a question as to whether there is any mortality benefit, and for who this might apply.
We discussed a patient who had a label of asthma and who had had 3 admissions with 2 intubations associated with a mixed acidosis. A sleep study showed nocturnal hypoxia. Spirometry showed a restrictive pattern. This patient in fact had kyphoscoliosos. We considered when to give NIV in kyphoscoliosis – guidelines are lacking.
We also discussed a patient with deteriorating MND with diaphragm weakness. A useful test in the clinic is a lying VC. When should we consider NIV in MND? Expert advice should be sought, particularly as this is a decision for patient and clinical team to make together.In MND there is evidence of improved sleep quality and QoL and survival on NIV. Better results are gained if normal/moderately impaired bulbar function (rather than severe bulbar function) so timing for initiation in important. Importantly, guidelines suggest a SNIP <40% has 97% sensitivity for death <6/12!
- Reference ranges for SNIP have been published by a number of authors: Enright 1995, Uldry 1995, with some guidelines for use from Lofaso et al (although in practice when screening for respiratory muscle weakness in clinic not many people would do 10 sniffs).
- Velasco et al 2002 showed that the time spent <93% correlates with survival in MND.
A >30% fall from sitting to supine VC is good measure of diaphragmatic weakness. This is a great screening test that can be done in any clinic without specialist equipment. Remember that pCO2 is not a great indicator of early respiratory muscle weakness.
Look for:
- symptoms of sleep disordered breathing
- thoracoplasty, cor pulmonale, abdo paradox, neuromuscular disease
- Spirometry
- Blood gas
- Overnight oximentry
- SNIP/MIP/MEP where available
We finished the day on a quiz! Sorry, you had to be there.

Discussion
Trackbacks/Pingbacks
Pingback: News and Opportunities | Resp NET - June 28, 2016