An enthusiastic group of trainees met at Homerton Hospital in July, keen for interaction and participation! Many thanks to Dr Angshu Bhowmik for co-ordinating the day, and for speakers who travelled from other hospitals to give talks.

Intro
Dr Angshu Bhowmik, started the day with a welcome refresher on the indications, contraindications and basic mechanics of NIV. He encouraged us all to look out for the new NIV audits, and the NCEPOD review, which is very likely to lead to changes in practice. It is possible that NIV will become Consultant led everywhere (as it is already in some hospitals), but this may look different in different places. Acute physicians are likely to be involved as well as Respiratory physicians in order to cover rotas.
We ran through some cases, and reviewed the causes of both T1RF and T2RF with ABG results. The usual cause is inadequate alveolar ventilation, but this may occur due to a number of different causes (examples only – not a comprehensive list. Those with stars are indications for NIV which could be considered outside a level 3 environment):
- central respiratory depression
- OHS*
- drugs eg opiates
- CNS trauma, haemorrhage or infarct
- tetanus
- neuromuscular weakness*
- Guillan-Barre syndrome
- Primary myopathies
- Myaesthenia gravis
- Polio
- cervical cord injury
- lung/airway disorders
- ARDS
- COPD*
- severe asthma
We reviewed respiratory physiology in relation to hypercapnia, particularly focusing on the way in which supplemental O2 may reduce hypoxic vasoconstriction and causes poorly perfused lung CO2 to return to the circulation increasing pCO2. Although often discussed, a lack of hypoxic drive is not much of a factor.We also revised the Haldane effect (deoxygenation of the blood increases its ability to carry carbon dioxide) and the Hb-CO2 dissociation curve. There is a nice explanation online, by DundeeChest , with animations. This article is also useful (found via lifeinthefastlane.com):
- Abdo, Wilson F., and Leo MA Heunks. “Oxygen-induced hypercapnia in COPD: myths and facts.” Critical Care 16.5 (2012): 1.
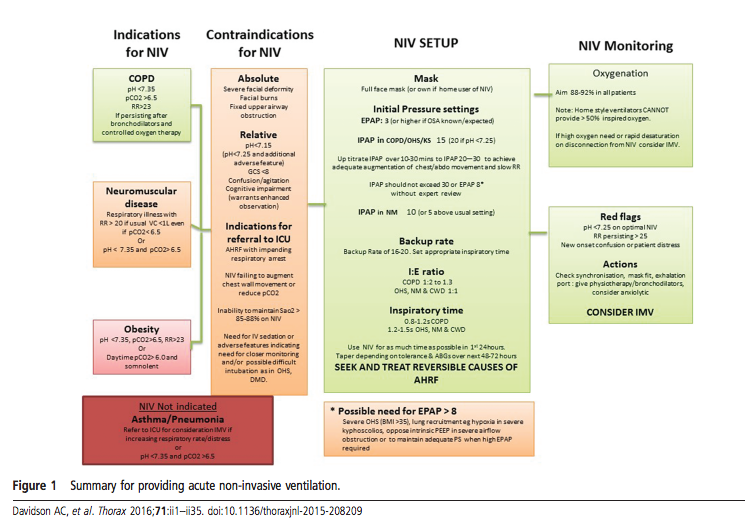
In the treatment of T2RF we aim for PaO2 >6.6kPa without a fall in pH <7.26. We reviewed the indications for BiPAP as per BTS guidelines (updated in 2016): PaCO2 >6 pH <7.35 despite max medical therapy (in reality trigger re: pCO2 more often 8 as many patients have chronic T2RF and tolerate higher pCO2 without acidosis – as ever, guidelines must applied appropriately to the individual in front of you). In any patient with a pCO2 persistently >8 consider domiciliary NIV (see this recent review from Feb 2016 on clinical trials in home ventilation, Hodgson & Murphy, 2016).
We discussed the need to always document resus status before starting NIV – audits show that this is only done in 50% cases!
We considered how to adjust ventilator settings to optimise NIV:
- If leak is 30-60L then monitor, if >60 then adjust. Make sure mask fit is good – there is a balance to be struck between tight mask vs optimal flow.
- Not everyone is comfortable with adjusting I:E ratios. The updated BTS guidelines helpfully includes I:E ratios advised for different conditions.
- Ramp – start at same as EPAP. Duration depends on patient anxiety level, but is usually 5min. It allows a period of time over which pressure increases, rather than initiating at target pressure. Can be useful for patients who need high pressures (more for domiciliary setting than acute). Ramp only happens when the machine is started. Alternatively you can stand by the machine and increase pressure gradually – more likely to use this method in the acute setting.
And James volunteered to try it out!

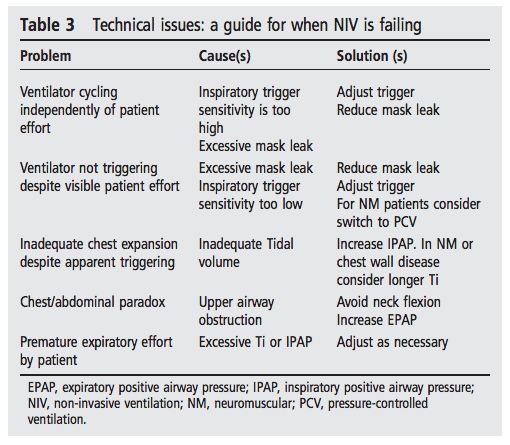
Helpful tips from the BTS guidelines:
A London NIV forum has been setup. We hope that this will help to harmonise practice across the region, for patient benefit, and as this will be very welcome to rotating trainees.
The flow diagram from the BTS guidelines 2016 is also very useful:
Sim sessions
We moved to the Sim centre to put our knowledge into practice and were faced with a distressed patient with an exacerbation of COPD with acidotic T2RF – pH 7.24. Bicarb was raised indicating acute on chronic respiratory failure. The patient had already had optimal medical management with nebs, steroids, antibiotics, and O2. A CXR had already been done to exclude pneumothorax.
Anna expertly assessed the patient, and initiated them on NIV. Rishi later took over and reassessed when the patient was not improving sufficiently, bringing structure and a calming manner. Rory played the part of the not so helpful ICU SpR.

In the debrief discussion we focused on non-technical factors, including managing the stress of the team and the situation. Breathlessness makes people stressed! One way to maintain control of a situation is to speak slowly – giving the impression of control can calm a situation. Keep instructions and summaries simple and structured. The sim session was very useful and highlighted the value of sim training for non-arrest situations e.g. NIV.
Other discussions included the relevance of the rise time (for each breath how long it takes to get to peak I pressure), and whether to use benzodiazepines to facilitate NIV use for anxious patients. The clear consensus was that this was only safe in ICU. Outside ICU, it may be justified if NIV is the ceiling of care, or to facilitate palliative use of NIV (if this is appropriate) but caution must be employed.
OSA
Dr Himender Makker from UCLH and N Mid gave us an update on treatment of OSA(S). Some of the audience were disconcerted to hear that both short and long sleep duration are association with an increased risk of death in a systematic review and meta-analysis of 21 studies – aim for 6-8hrs a night for a long life! There has been an explosion of research into sleep with over the last 40years, which has also seen new diagnostic categories of sleep disorder defined by ICSD-3 categories.
- Sateia, Michael J. “International classification of sleep disorders-: highlights and modifications.” CHEST Journal 146.5 (2014): 1387-1394.
Suspicion of OSAS may come from symptoms, physical features, or screening questionnaires. Traditionally, the ‘typical’ patient was thought to be obese, with a large collar size ie >16 inches (40cm), waist circumference >104cm. However, crania-facial features (such as micro and retrognathia) may also be very relevant, in the absence of obesity. There are diagnostic features which may be apparent by looking in the mouth including a large tongue (eg in acromegaly), large uvula, large tonsils. Mallampati score is a useful brief assessment.
- Epworth score is useful for tracking symptoms, but not for diagnostic screening.
- Berlin questionnaire – validated in primary care. Not easy to use or score. Only really used in research.
- STOP-BANG – easy to use. Useful in pre-op setting for screening. High risk >3.
Diagnosis is then based on a sleep study. The AASM and SIGN diagnostic criteria define OSAS is symptoms + AHI >5. Clinically significant OSAS >15 (generally).
- Overnight oximetry is often the initial investigation. It has a sensitivity 87% and specificity 65% if dip 4% >10dip/hr (equivalent to AHI >15). Other criteria include % sleep time <90% >10% time.
- Polygraphy (egVisilab) is oximetry + HR + video (movement) + snoring index (decibels) which provides additional info. Apnoea may not to lead to desaturation so false negatives can occur on oximetry (e.g. dependant on baseline sats, apnoea duration etc).
- Multichannel e.g. Somnolgica has a chest and abdominal band, and gives flow as well as Sats, HR, audio.
- PSG: includes EEG, EMG. Not required for most cases – really only for neurological conditions or those that are more difficult to diagnose. Gives sleep stage in addition to other information. Useful if sleepy but normal oximetry and AHI. e.g. Upper airway resistance syndrome, periodic limb movement syndrome, narcolepsy, poor sleep hygiene (actigraphy useful for this).
Treatment of OSAS is not just aimed at improving daytime somnolence – cardiovascular complications are also relevant. The following study was conducted when tracheostomy was the treatment for OSA!
- Partinen, Markku, Andrew Jamieson, and Christian Guilleminault. “Long-term outcome for obstructive sleep apnea syndrome patients. Mortality.” CHEST Journal 94.6 (1988): 1200-1204.
The Wisconsin Sleep Cohort Study followed 1500 state employees, initially over 4 years. It was a good quality observational cohort study, published in NEJM. There was a dose–response association between sleep-disordered breathing at base line and the presence of hypertension four years later that was independent of known confounding factors. Later systematic reviews and meta-analyses have shown a consistent relationship between untreated OSAS and cardiovascular outcomes, including hypertension, and also MI and stroke.
Mandibular advancement devices may be ‘off the shelf’ or custom made. They move the lower jaw forward by about 1cm to move the tongue. This reduces AHI by 50% in those who tolerate them, which may be enough to improve symptoms. Compliance is good (particularly in those not tolerating CPAP).
A crossover RCT of mandibular advancement devices found that “Non-adjustable MADs achieve clinically important improvements in mild to moderate OSAHS and are cost-effective.” Semi-bespoke were compared to devices fitted and made by dentists.
Possible future treatments include upper airway muscle stimulation via hypoglossal nerve. The trial recruited patients with moderate to severe OSA who were CPAP-intolerant. Expensive, invasive. At the end of the session we also discussed the place of auto-CPAP, chipped machines, the use of compliance data and remote monitoring.
ILD in 2016: where are we now?
Dr Bhagy Jayaraman provided an update on ILD. The UK incidence of ILD is 50/100,000 (30,000/yr), and of IPF is 8/100,000. 40% are associated with CTD (10-40% are RA, 70-90% systemic sclerosis). Life expectancy is between 2-15yrs, worse in those with IPF.
The classification of ILDs has changed multiple times over the years. The newest classification has just 4 groups:
- ILD with a known association (CTD, drugs, occupational)
- Granulomatous (sarcoid, HP)
- Idiopathic (split into major, rare, and unclassifiable)
- Miscellaneous (LAM, Histiocytosis X)
Major causes include: IPF, NSIP, OOP, RB-ILD etc
There remain debates regarding the place of tissue diagnosis in the diagnostic pathway. In one study, 20/46 patients diagnosed with IPF according to guidelines had a subsequent diagnosis of chronic hypersensitivity pneumonitis.
- Morell, Ferran, et al. “Chronic hypersensitivity pneumonitis in patients diagnosed with idiopathic pulmonary fibrosis: a prospective case-cohort study.” The Lancet Respiratory Medicine 1.9 (2013): 685-694.
BAL can be useful in HP and for CD4/CD8 ratio. However, it is not specific enough to replace biopsy in difficult cases. Previously surgical lung biopsy (VATS) was recommended for those with non-classical IPF. TBB is inadequate for the diagnosis of fibrotic ILD diagnosis as it has a low sensitivity (30% for expert pathologists), and low negative predictive value (50%). Findings consistent with alternative diagnosis (e.g. COP) does not rule out UIP.
Cryobiopsy is under investigation at UCLH (and other centres). Is this the future? It has a lower risk than VATS, and higher accuracy than TBB. Data is limited. There is a 10% pneumothorax rate, with prolonged air leak in 0.1%. It is a day case procedure, but an overnight stay is required if there are complications – some need a drain. Standardisation is needed for procedures. Should it be done under deep sedation or conscious sedation? How many samples is optimal?How many segments/lobes should be sampled?
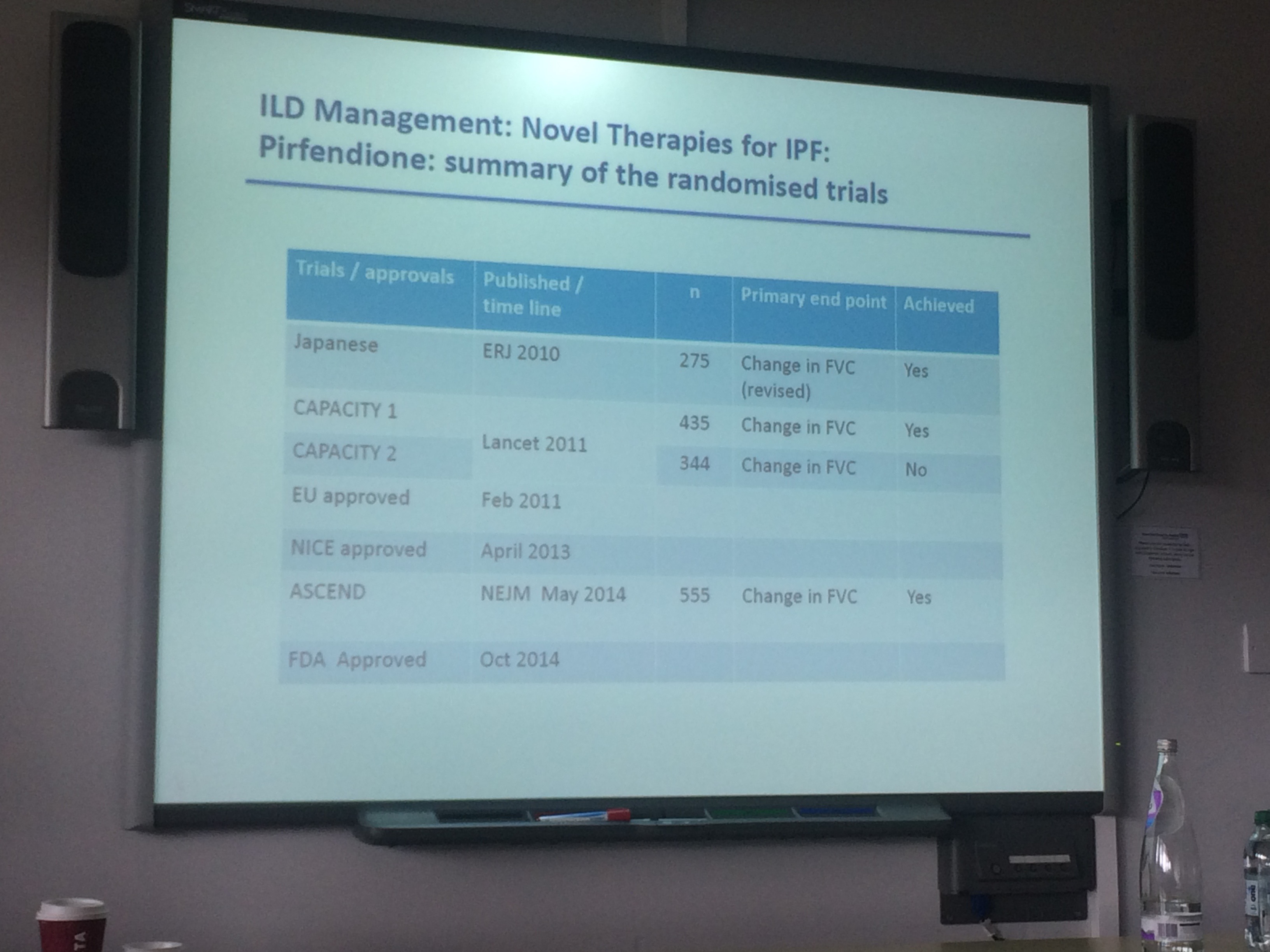
There have been a number of drug trials recently – all end points are FVC % change.
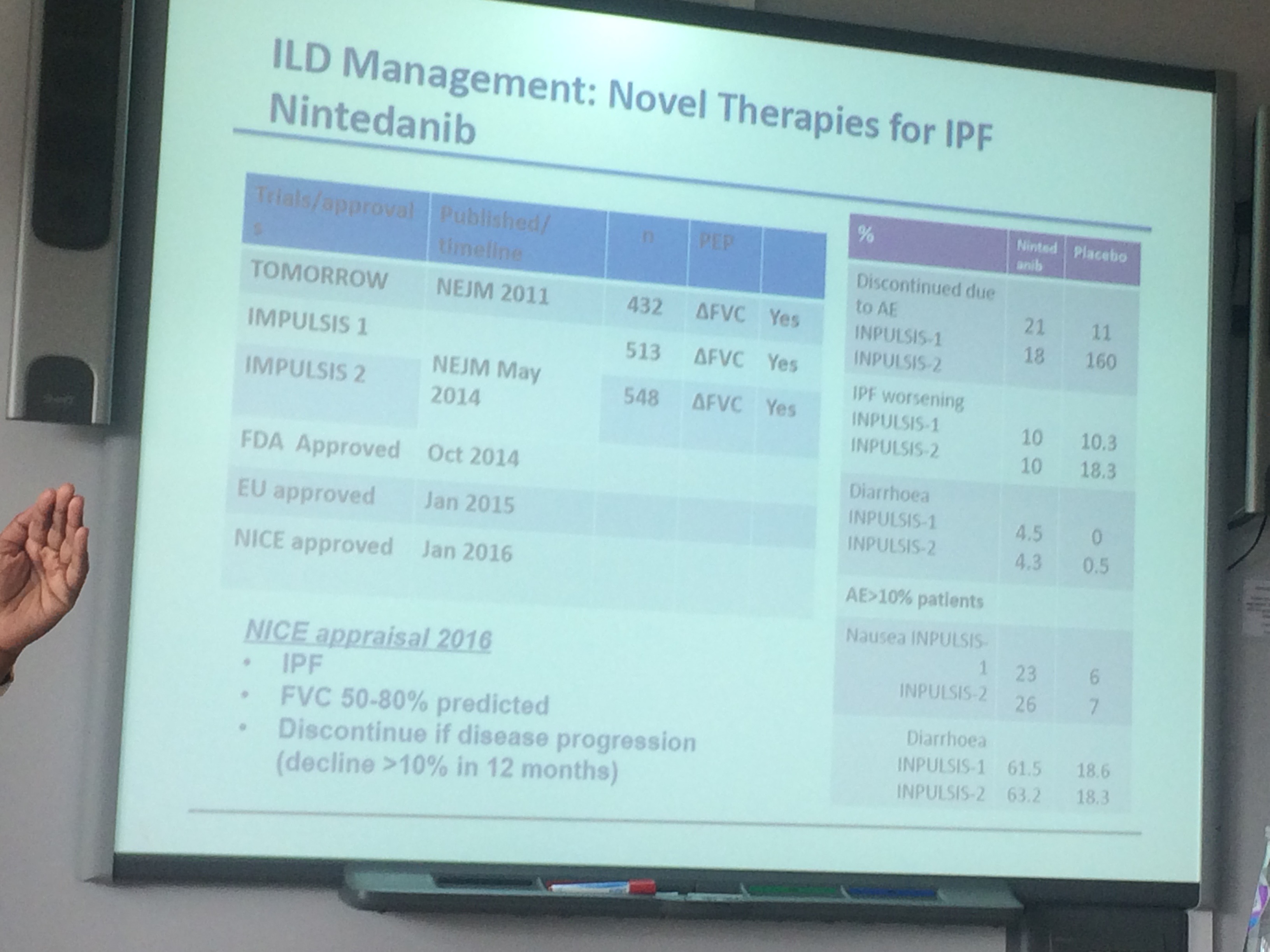
- NICE approved Nintedanib in Jan 2016 following the INPULSIS study.
- It was hoped the extended PANTHER study (without the triple therapy arm) would show evidence for NAC but there was no difference in FVC at 52 weeks.
A few questions were discussed at the end of the session. IPF exacerbations may be treated with high dose Pred or IVMP pulsed for 3/7. Immunosuppression is favoured for CTD-ILD e.g. MMF. Biomarkers in ILD would be useful in diagnosis, prognosis, and treatment tailoring. FDG-PET SUVmax is a potential biomarker in ILD which could be measured pre and post treatment? As yet unproven.
Medicolegal matters
A team from Drake and Case Law solicitors, accompanied by a barrister, Ms Helen Nugent from No.18 Barristers’ Chambers ,came to give us the low down on medicolegal matters. As doctors we may attend court as a witness, expert witness, or defendant. The session focused on civil cases. We all hope to avoid criminal charges!
We took a brief look at medicolegal reports. These may be written for example to document the nature of injuries sustained, the cause of injury, the effects/prognosis of the injury. They must be compliant with civil procedure rules. The duty of the doctor writing the report is to the Court, not the paying party. Key obligations are:
-
- independence
- objectivity not advocacy
- confirm any assumptions
- to stay within expertise
Even if a case is brought against you, the probability of attending court as a defendant is low – 50% do not reach court, and 95% settle. It is much more likely that you will have to provide a witness statement.
It is worth remembering that to be negligent it must be established:
- that there is a duty of care
- that the duty of care has been breached
- there was a causal link between the breach of duty and harm
- the harm was not too remote from the incident
Relevant case law for determining whether a duty of care has been breached includes Bolam and Bolitho.
- Bolam v Friern Hospital Management Committee [1957] laid down the typical rule for assessing the appropriate standard of reasonable care in negligence cases involving doctors. A patient was voluntarily an inpatient at a mental health hospital and underwent ECT. He was not given muscle relaxant and was not restrained. He suffered injuries including a fractured acetabulum. The use of muscle relaxants was not universal, with a significant body of opinion being against their use. Similarly, some doctors believed that restraints increased fracture risk. The Bolam test states that “If a doctor reaches the standard of a responsible body of medical opinion, he is not negligent”. In this case the doctor was not found negligent as, even though opinion was divided, he acted in line with practice of a significant body of medical opinion.
- Bolitho v. City and Hackney Health Authority [1996] came later. This case ruled that for any individual decision risks and benefits must be weighed up by the doctor, and that it may be possible for negligence to occur even if the doctor was conforming with a body of expert opinion. In this particular case the doctor did not see a child, as their pager was broken. It was argued that if the child had been intubated earlier, they would have lived. The defendant argued that they were not negligent as, even if they had seen the child earlier, they would not have intubated the child, and that this was in line with a body of medical opinion. The ruling stated that “the court would hold a practice that was in conformity with a sound body of expert opinion to be negligent only in “a rare case”“. In this case the doctor was not found to be negligent as not intubating at that point would not have been a negligent way to act.
The standard of proof for negligence is the balance of probabilities that the action of the doctor resulted in an adverse event.
A common reason for claims is delay in referral or treatment. Such a delay can have a profound effect on a patient’s quality of life. Political and economical factors are relevant in such cases, but responsibility lands at the door of the treating physician.
Top tips when in trouble:
- Tell the truth so you don’t have to remember anything!
- Avoid making assumptions – rely on contemporaneous records/notes (a good reason to always make good notes)
- Don’t let supervisors/seniors influence you (it is important to write you own statements, and get independant advice)
- Don’t be afraid to make concessions (an apology is not a blanket admission of guilt)
- Prevent exposure in court (make sure your witness statement is clear and includes all relevant info)
- Make your evidence your own
LJ and Zaheer bravely volunteered to be questioned by solicitors and barristers in role plays. LJ was cross-examined as a defendant on a charge of negligence (something she hopes never to repeat). Zaheer was questioned as an expert witness. Both did very well under pressure and had good feedback from the lawyers. Neither fell into the trap of going outside their sphere of knowledge or expertise. Well done! This was a really valuable session so thanks to all those who arranged the outside speakers.
Inhalers
The last session of the day was from Jon Bell. A Radiographer by training he was interested in physics, particularly MRI. But he started working for a drug company and became interested in devices, rather than drugs. He is now very knowledgeable about (some may say obsessed with!) inhaler devices, and shared this with us, with a particular focus on optimising inhaler technique.
He presented some data from an ATS(2002) poster by L. Pearce. Do Health Professionals Have sufficient knowledge and skill to teach optimum inspiratory flow? The answer was no! The Accuhaler, Evohaler and MDI were tested. <1% full dose with MDI. A poster at the BTS 2010 showed slightly better results amongst a team in Milton Keynes who had been trained. (Baverstock M).
We examined what is meant by ‘Poor inhaler technique’, such a commonly quoted problem. What it leads to is lower than expected delivery of drug to target site, reduced benefits, increased deposition outside target sites, and increased risk of side effects.
- Al-Showair, Raid AM, et al. “Can all patients with COPD use the correct inhalation flow with all inhalers and does training help?.” Respiratory medicine 101.11 (2007): 2395-2401.
In this study trained pharmacists check technique. Inhalation was too fast for pMDI and too slow for DPI.

A peak inspiritory flow meter – how have we lived without it until now?
A Peak inspiratory flow metre is a very useful tool to check technique. As we discovered when checking our own inhaler technique!
Different techniques are needed to optimise drug delivery to the lungs through different devices. In order to support our patients in getting optimal use of their devices we must understand them better ourselves.
- DPI: need to breathe powder in down to lungs. Small quantity of large particles – needs energy to break up particles to make aerosol and get into lungs rather than upper airways. (Accuhaler, Turbohaler, Handihaler, Twisthaler).
- MDI most common: problem timing/synchronisation. Common to breathe in too fast. Shorter window to synchronise inhalation and drug release. MDI technique should be slow and steady. Should be <60L/min PIF. (range in room 80-320). Still need to go slow with spacer. Particles hit back of throat, With practice most of us achieved 40!
Breath activated MDI – trigger at low flow so still work best with long, deep, gentle inhalation. Remember, a spacer shouldn’t whistle.
Air flow is different through different devices, yet another reason why it is important to match the right device for each patient. Data on the mean resistance of MDIs and DPIs is not easily accessible as companies don’t always release the data on resistance. The “Easyhaler” has a rather ironic name as it has high resistance.
In general drug delivery to the lungs with good technique is around 20%. This falls to just 5% with poor technique! The benefit of improving technique is that a lower dose can be used, meaning less steroid, and fewer side effects.
We covered some other factors related to inhaler design, including a physics refresher on flow, mass and velocity. Lung deposition from pMDIs is influenced by inspiratory flow. Therefore it may be beneficial to learn to breathe gently first then add in the inhaler. Spacers are useful for a number of reasons. They reduce the need for co-ordination, so get better results. They also remove charge.
- Newman, S. P., et al. “The effects of changes in metered volume and propellant vapour pressure on the deposition of pressurized inhalation aerosols.” International Journal of Pharmaceutics 11.4 (1982): 337-344.
- Roller, C. M., et al. “Spacer inhalation technique and deposition of extrafine aerosol in asthmatic children.” European Respiratory Journal 29.2 (2007): 299-306.
Multiple new inhaler devices have been added to Jon’s expanding bag of tricks!
A number of new devices have recently become available – confusing for both clinicians and patients!
When reviewing the literature on new devices it is important to remember that ‘delivered dose’ usually means that delivered to the mouth, not the small airways. Consideration of inhaler device, required inspiratory flow, resistance and other factors related to technique is important. An ideal DPI would have the same drug delivery at low and higher effort. We await such a device!
Key messages from this session were:
- Know your devices – MDI or DPI?
- Internal resistance affects speed of inhalation
- Speed of inhalation affects DPI device efficacy
- Speed of inhalation and particle size affect how much drug is deposited in the lungs (and how much int he mouth/throat)
- Know what optimal technique is for each device type
- GENTLE for MDI (as it creates the aerosol for you)
- FORCEFUL for DPI (as needs energy to create aerosol)
- Get enthusiastic and knowledgable about inhaler technique in order to teach it better
- Make the discussion of inhaler technique relevant to the patient: better technique = better disease control + lower steroid dose = fewer side effects
- Use training adjuncts – they are great!
There is evidence, from an Isle of Wight study, that focusing on technique only with no other changes made to care, led to reduced use of oral steroids and hospitalisations. The Isle of Wight now has the lowest standardised admission rate for asthma in the UK! Impact! See NICE “shared learning database” for further information on this project.
We finished the day in the pub – a key part of any training day where essential information is exchanged. Don’t miss drinks next time!

Discussion
No comments yet.