In January we met at St Bartholemew’s Hospital for a pan-London Training Day on Asthma and Allergy. Barts has a specialist allergy service offering desensitisation and biologics, and also a severe asthma service, including specialist physiotherapist, dietician, psychologist and access to biologics.
Allergy testing and treatments
Dr Runa Ali started the day by updating us on changes within the specialty. There is now a CCT in allergy which is good news as allergy is common and understaffed as a speciality. In the House of Lords Science and Technology Committee report on allergy 2006-7 it was noted that there is a lack of specialist allergy services, and a lack of teaching about allergy in medical school. 30% of the Uk population has allergy of some kind and many more have intolerances. Both allergy and anaphylaxis are dramatically increasing, reflected in the fact that there has been a 7x increase in admissions over 10yrs. Since there is a paucity of allergy services, and patients do not always know where to go for help, there is a lot of pseudoscience out there claiming to be allergy diagnostics and treatments. You can part with large sums of money to undergo tests such as hair analysis, VEGA testing, and kinesiology, which all lack evidence
Want to know more about allergy? Take a look at www.bsaci.org for guidelines, study days, conferences and more.
When to refer to a specialist allergy service:
– difficult rhinitis – for desensitisation and ENT assessment
– food and drug allergy – consider complex testing and specialist dietician advice
– venom allergy – desensitisation
– anaphylaxis – Ix and adrenaline auto injector training (see NICE guideline)
– severe chronic urticaria/angioedema – consider biologic therapy
– not eczema! patch testing is done by Dermatologists
Allergy means different things to different people. To us (doctors) it is IMMUNOLOGICAL:
– type 1 immediate IgE mediated
– type 4 delayed cell mediated
Allergy develops after sensitisation (type 1 hypersensitivity) – IgE antibodies are produced by B cells. It is possible to be sensitised and have no symptoms – atopy. A useful term to use that is familiar to patients is ‘carrier’. This is common in families.
How to diagnose allergy – it’s all in the history. The negative predictive value of history alone is 95%. Testing merely confirms or excludes a suspect from the history. Tests are not helpful alone. 1/3 population is atopic.
Type 1 hypersensitivity. The early phase reaction due to histamine release direct from mast cells peaks within 15min, and is gone within an hour. A late reaction can occur 6hrs later due to T cell eosinophil reaction. These people are ‘dual responders’. This is why patients must stay in hospital after anaphylaxis for 6hrs in case of late phase reaction. They also need a course of steroids (3/7 is sufficient).
Timing of symptoms is very important. Eg eat peanuts/seafood/MSG/alcohol…
5 seconds too quick for allergy – aversion
5 minutes lip swelling – just right for allergy
4hrs D&V – not allergy, but may be scrombotoxin
18hrs – too late for allergy, more likely food poisoning e.g. salmonella.
Anaphylaxis is laryngeal oedema, bronchospasm AND/OR fainting, light headededness, CV collapse, LOC. With other symptoms e.g. itching.
Tests:
- Specific IgE – there are over 450 food and inhaled allergens that have SpIgE available (good for food items, or if no access to SPT). Importantly, these tests can be done whilst on antihistamines. £25/go. Also need to do total IgE to put in context.
- Skin prick testing – the patient must not have had antihistamines for 48hrs before test. A positive test is 3mm more than -ve control (wheal). This is essentially an in vivo reaction – mast cells in skin release histamine. This test can also be done with fresh foods (as well as bought-in pre-made allergens)
- Components testing – molecular tests against different components are useful to help risk assess and devise management plans. Some components are heat labile/sensitive. A good example is egg proteins. Ovomucoid, Ovo-albumin. Patients may be able to eat cake but not mousse.
- ISAC (immune solid-phase allergic chip) – is a panel of many allergens. It may be cheaper to run a whole panel in a patient who appears to have multiple food allergies.
- Drug allergy tests – intradermal testing 0.03ml.
- Provocation challenge – double blind placebo controlled challenge (gold standard for food/drug challenge) – need to do risk/benefit assessment, and have an anaphylaxis kit, crash trolley etc.
- Histamine release test – if it is not safe/possible to do a provocation challenge then this is a useful new alternative. It is a blood test which measures the release of histamine in vitro from basophils after addition of the allergen (drug). It is specific, but not necessarily sensitive, and false negatives do occur. It is helpful in complex cases.
Update on specialist treatments
- Desensitisation is a really useful treatment for allergic rhinitis. Unfortunately current subcutaneous agents are contraindicated in asthma. A newer sublingual version may be safe for asthmatics. (see Alves, Bernadette, et al. “Allergen injection immunotherapy for seasonal allergic rhinitis.” Cochrane Database of Systematic Reviews 1 (2000)).
- Biologic therapy: Xolair (used in asthma) is also approved for chronic urticaria – it works by removing free circulating IgE, and leads to down regulation of IgE receptors on mast cells.
- NICE guidance was most recently updated in 2011. Emerade (0.5mg), Epipen (0.3mg), Jext (0.3mg) are all brands of adrenaline autoinjector. 1/1000 = 0.5ml. There is the full 0.5mg in Emerade so this is recommended at Barts. Not only is it full strength but the needle is also longer, meaning it is more reliably im. Remember, always give 2 auto injectors to patients. Advise them to repeat the injection after 10min if they are no better or an ambulance has not yet arrived.

From wikipedia.org/wiki/Immunoglobulin_E
We discussed some cases of allergy and anaphylaxis which demonstrated the learning points from the earlier sessions very well. An important points was that it is possible to get a false negative SpIgE after anaphylaxis as IgE is consumed in the reaction. If the history is good it is important to repeat the test in 3 months.
Another case highlighted the important features which differentiate angioedema and anaphylaxis. Angioedema secondary to ACEi is not uncommon and many people are on these medications for IHD or HTN. If the history is clear, then an adrenaline auto injector is not required.
Rhinitis and beyond
Dr Stefan Lozewicz aimed to answer three questions in relation to rhinitis:
- What types of rhinitis are there?
- How do we manage rhinitis?
- What food allergies are associated?
He started with an illustrative case of a patient with a 3year history of nasal discharge, blockage, and sneezing between March and May. Antihistamines were some help but he remained symptomatic. The seasonal pattern means this is very likely to be tree pollen allergy leading to rhinitis. See guidelines:
- Scadding, G. K., et al. “BSACI guideline for the diagnosis and management of allergic and non‐allergic rhinitis (Revised Edition 2017; 2007).” Clinical & Experimental Allergy 47.7 (2017): 856-889.
Interestingly, if there is a warm winter it can shift the timing of seasons/allergy symptoms. What will happen with climate change? However, in general:
- June – July = grass
- March – May = tree pollen (birch most common)

Perennial rhinitis
- House dust mite (HDM) dermatophagoides pteronyssinus
Rhinitis should be classified as:
- Infective
- Allergic – seasonal, perennial (home & work)
- Non-allergic
- non-allergic rhinitis with eosinophilia (NARES)
- Drugs (aspirin, NSAIDS)
- Idiopathic
- Hormonal (pregnancy, hypothyroidism)
- Systemic/inflammatory: SLE, EGPA
- CF, PCD
The Patient Voice allergy survey from 2008 brought home the impact of rhinitis on quality of life. Although not life threatening, it should never be dismissed as a trivial problem. Sleep disturbance is a major issue, and school absence and sick leave can have major consequences.
- Valovirta, Erkka, Svein-Erik Myrseth, and Susanna Palkonen. “The voice of the patients: allergic rhinitis is not a trivial disease.” Current opinion in allergy and clinical immunology8.1 (2008): 1-9.
Having clarified the diagnosis and classification of rhinitis, we moved onto treatment. A systematic review on HDM avoidance measures shows mixed evidence.
- Nurmatov, Ulugbek, et al. “House dust mite avoidance measures for perennial allergic rhinitis: an updated Cochrane systematic review.” Allergy 67.2 (2012): 158-165.
9 RCTs looked at air filters and found a 50/50 chance of benefit. Acaricide and/or home cleaning – 2/2 RCTs found benefit. Mite impermeable bed covers alone 0/3 trials showed benefit.
The most effective medication for allergic rhinitis, according to a BMJ 1998 meta-analysis, is intranasal steroids. These are more effective than antihistamine tablets. Interestingly, they are also effective for eye symptoms. The first line treatment for mod-severe persistent symptoms is intranasal steroids.
- Sausen, Verra O., et al. “Management of allergic rhinitis.” The Journal of Pediatric Pharmacology and Therapeutics 10.3 (2005): 159-173.
When considering who to treat, it is useful to consider the definitions of terms used in guidance documents:
– Intermittent: <4 days/wk or <4weeks
– Persistent: >= 4days/wk for >= 4 weeks
Some patients may have concerns about long term steroid use. Systemic bioavailability is <1% for newer intranasal steroids e.g. Fluticasone furoate (Avamys) so this is not a concern and patients can be reassured. Budesonide, which is seldom used now, has much higher bioavailability.
What if optimal medication fails for allergic rhinits? Desensitisation is a ‘modern’ treatments which in fact was first published in 1911 in the Lancet. Patients with symptoms on allergen exposure, and SpIgE, whose symptoms persist despite optimal medical therapy should be considered for allergen immunotherapy. This may be via injection or sublingual.
Examples of injected immunotherapy:
- Pollinex Quattro – for grass pollen allergy, tree. Given as 4 injections at wkly intervals each year for 3 yrs before seasonal onset.
- Alutard SQ – tree mix, cat, dog, HDM. 12 sc weekly injections at inc dose then maintenance dose for 4-6/52 for 3 yrs.
This service is only available in a few centres, requires a 1hr stay for each injection, and carries a small risk (1-2/1000) of a systemic reaction (so ALS providers and a crash trolley must be available).
Sublingual immunotherapy:
- Grazax for timothy grass pollen. Start 4/12 before season. Every day for 3yrs. Taken at home.
- Lais for grass pollen, cat, HDM allergy. For seasonal 2 months pre-seasonal and through season, for 3 yrs. Twice/wk for 3 yrs for non-seasonal.
Oral allergy syndrome is a condition in which patients experience tingling in the mouth when they eat certain foods. eg apples, hazelnuts, peaches. Skin prick tests are usually positive to birch pollen. This is due to the fact that IgE antibodies cross-react with structurally similar proteins of other members of the plant kingdom. These are usually labile, and therefore broken down by heat/acid. So patients may be able to eat e.g. cooked apples without symptoms. These proteins are PRP-10 proteins and Profilin.
Non-specific lipid transfer proteins are a different class of proteins, which are stable to heat and digestive enzymes. Patients sensitised to these are more likely to have a systemic reaction. They are not oral allergy syndrome proteins and symptoms are not oral.
Antibiotic Allergy
Dr Runa Ali gave an up to date overview of antibiotic allergy. She encouraged us all to review the NICE guideline:
- Dworzynski, Katharina, Michael Ardern-Jones, and Shuaib Nasser. “Diagnosis and management of drug allergy in adults, children and young people: summary of NICE guidance.” Bmj349 (2014): g4852.
This is a highly relevant to both Respiratory and GIM practice:
- Up to 15% of hospital inpatients have their stay prolonged due to an adverse drug reaction (this includes C Diff as well as allergic reactions).
- Up to 10% report Penicillin allergy – true figure is only 1% of population.
- ‘Pen allergy’ patients are more likely to receive 2/3rd line antibiotics including 3rd gen cephalosporins, vanc etc.
- Drug allergy is the commonest cause of death overall from anaphylaxis. Antibiotics are second to anaesthetic agents.
National Reporting and Learning system. 2005-2013 – most cases have a documented allergy.
Dr Ali talked through a case of penicillin allergy to illustrate the problem. A useful test to consider post-exposure and reaction is SpIgE to penicillin V and ampicillin. The patient needs to have had fairly recent exposure to be useful. If positive this is diagnostic of penicillin allergy.
TELL THE PATIENT. Tell them what alternative antibiotics they can have. Tell the patient to get a medic alert bracelet. Mark the notes, add an alert (to the EPR), and tell the GP. A 10% cross-reactivity with cephalosporins is quoted, but in reality it is much less than this – more like 1% but individuals still need to take care. The side rings differ in penicillins and cephalosporins. Penicillin side chain changes type of penicillin (benzylpenicillin, amoxicillin, ampicillin). What is the allergy to?
In patients who it matters (e.g. bronchiectatics who need lots of antibiotics) they need further investigation of allergies, in a specialist allergy service.
- IgE mediated immediate ADR (adverse drug reaction) is anaphylaxis, urticaria or asthma.
- Non IgE mediated delayed ADR occurs within 6-10 days of initial exposure, 3 days of 2nd exposure.
Assessment includes:
1. history – not always available
2. formal investigation including provocation test. This is highly protocolised and occasionally dangerous! It must only be undertaken in an appropriate specialist service.
Dr Ali invited all trainees to come and visit the allergy service – but please email.
Severe asthma
Dr Paul Pfeffer talked to is about asthma. 5.4 million people have asthma. Every day 3 people die due to an asthma attack. 2/3 of these deaths are preventable. However, most deaths occur in mild-moderate, rather than severe asthma.
What is severe asthma? This term should be applied to those who have symptoms, exacerbations, and inflammation despite appropriate treatment with steroids etc. This group need assessment for biologics.
What is difficult to control asthma? This term should be applied to those whose asthma is not controllable due to other factors. This may be because the diagnosis is wrong, there is poor compliance, or other issues.
There is of course some overlap.
- Chung, Kian Fan, et al. “International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma.” European respiratory journal 43.2 (2014): 343-373.
Guidelines state that patients must already be on the on highest dose ICS (ie Symbicort 400/12 TT BD or equivalent with pick up of 2 inhalers/month),
and have poor symptom control (ACQ) and/or frequent severe exacerbations (2+ systemic OCS in 1yr). Other criteria are: any intubation in last 10yrs on high dose ICS; FEV1<80% fixed airway disease; those who become symptomatic if try to wean oral steroids.
- Haldar, Pranab, et al. “Cluster analysis and clinical asthma phenotypes.” American journal of respiratory and critical care medicine 178.3 (2008): 218-224.

From Haldar et al 2008
Haldar et al identified clinical phenotypes with cluster analysis. Important findings were that two phenotypes, early-onset atopic; and obese, noneosinophilic, were common to both a primary care population and a tertiary population. Two clusters characterized by marked discordance between symptom expression and eosinophilic airway inflammation (early-onset symptom predominant and late-onset inflammation predominant) were specific to refractory asthma.
Overlapping diagnoses make asthma management challenging: COPD, bronchiectasis, infective bronchiolitis, post-infective bronchospasm, VCD, hyperventilation syndrome, eosinophilic bronchitis, hyperIgE syndrome, NTM bronchiolitis….
Asthma is a SYNDROME at best, rather than a disease.
- O’neill, Stephen, et al. “The cost of treating severe refractory asthma in the UK: an economic analysis from the British Thoracic Society Difficult Asthma Registry.” Thorax 70.4 (2015): 376-378.
- Sweeney, Joan, et al. “Comorbidity in severe asthma requiring systemic corticosteroid therapy: cross-sectional data from the Optimum Patient Care Research Database and the British Thoracic Difficult Asthma Registry.” Thorax (2016): thoraxjnl-2015.
An economic analysis from the BTS difficult asthma registry showed that side effects due to steroid use are a big cost. So getting people onto biologics and reducing steroid use is important. There is specialist commissioning for ‘high cost drugs’ e.g. omalizumab. In London there are severe asthma services at Barts, Guys, and the Brompton. The Barts specialist asthma service MDT is on Monday afternoons – all trainees are invited to attend. The MDT includes Respiratory Consultant, Allergy Consultant, ENT, physio, psychology, pharmacist, dietician, and specialist nurses. Personalised management plans are agreed, based on endotyping. This leads to improved care. Outcomes are audited.
In the severe asthma service, the sructured assessment is protocolised, based on Robinson et al 2003.
Multiple inhalers confuse asthma patients. This is a problem as the only LAMA licensed for asthma is the Tiotropium Respimat and there are no other inhalers using the same device.
What is acceptable adherence? 70% prescription refill? 80% refill? To get accurate refill data, we currently ask GP pharmacists for data. An alternative is to use smart devices.
There is a high incidence of breathing pattern disorders in asthma. It is important to identify and treat these disorders to avoid unnecessary pharmacological treatment escalation.
The unified airway hypothesis shows that there is a need to treat nose to get the lungs better in asthma. There are both neuronal and immunological mechanisms that link them.
- Lipworth, Brian J., and Paul S. White. “Allergic inflammation in the unified airway: start with the nose.” Thorax 55.10 (2000): 878-881.
Physiotherapy Assessment and Management
Hannah Hylton presented the many roles of the physiotherapist in asthma management, and her role in the Barts severe asthma service.
Airway clearance
ACBT is widely used and is more effective than just cough and clear. The aim is to
open up channels in collateral ventilation, and get airflow behind phlegm to clear it.
It involves thoracic expansion exercises, and breathing control. Then Huffing is the key to clearance. See bronchiectasis.com.au for great videos on physiotherapy techniques.

From bronchiectasis.com.au/
Autogenic clearance is tricky to teach. The patient needs to engage well. It is a technique used more in CF than asthma.
Adjuncts to airway clearance can be very useful. These include PEP (positive expiratory pressure) therapy, oscillating therapy, nebuliser therapy, gravity assisted drainage, Acapella, Aerobeaker manual therapy….
Activity and exercise. In the UK 1 in 4 adults are inactive, doing <30min/wk physical activity. Exercise avoidance is high in the asthma population. Adults are recommended 150min/wk activity in blocks of 10+ minutes. Social factors are highly relevant; longterm unemployed most likely to be inactive (37%) compared to professionals or managerial roles (17%). When counselling patients, the focus should be on combatting inactivity, rather than intensity or duration of exercise.
Breathing pattern disorder has recently been reclassified into a number of patters.
- hyperventilation syndrome
- periodic deep sighing
- thoracic dominant breathing
- forced abdominal expiration
- thoraco-abdominal asynchrony
9.5% general population have breathing pattern disorder, and 20% children and teens (40% if they have asthma).
There is no gold standard for diagnosis of BPD. Diagnostic methods include: a Physiotherapist assessment looking at resp flow, freq, volumes; the Nijmegen questionnaire (only validated in exercise induced hyperventilation syndrome); Hyperventilation provocation test; ETCO2; Breath hold time.
When examining the patient, take note of: posture, noisy/quiet breathing, nose/mouth breathing, accessory muscles activated, RR.
Treatment aims to achieve breathing retraining. There is limited evidence for any specific intervention over another:
- Education – feeling validated and believed
- Buteyko methods – nasal breathing and increasing controlled pauses
- Papworth method – diaphragmatic breathing with emphasis on controlled slow nasal breathing, reducing minute volume
- Relaxation techniques
- PR
- Yoga
- Psychology input
- Social prescribing
Locally we have a great Singing for Breathing group, who meet at the Royal London Hospital each week. Singing is great for lung health so do encourage patients to attend.
Severe acute asthma in the ICU
Anthony Bastin from the critical care team at Barts spoke to us about severe acute asthma in the ICU. He highlighted the NRAD report from 2014 which examined 195 cases in depth, and the concern that asthma still kills.
- Gibbison, Ben, et al. “Ten years of asthma admissions to adult critical care units in England and Wales.” BMJ open 3.9 (2013): e003420.
In this series of 11948 cases, length of stay in critical care was 1.8 days (0.9-3.8). LOS in hospital 7 (4-14). Critical care survival was 95.5% (there were 539 deaths). Hospital survival was 93.3% (763 deaths). Study limitations were that there was no cause of death recorded and no admission details so there is limited learning from this study on why those that died, did so.

From BTS/SIGN guideline
There are a number of factors that have been identified, which put patients at higher risk of a near-fatal or fatal asthma exacerbation.
From a critical care perspective important parameters are: ‘normal pCO2’ means life-threatening asthma attack.
Anyone who fits this criteria should be escalated to critical care. We were encouraged to escalate to a Consultant if not getting any joy from ICU/anaesthetic SpR…
Magnesium is commonly given in acute severe asthma. The 3Mg trial was an RCT of >1000 patients in ED departments across the UK, and showed that this treatment lacks evidence.
- Goodacre, Steve, et al. “The 3Mg trial: a randomised controlled trial of intravenous or nebulised magnesium sulphate versus placebo in adults with acute severe asthma.” (2014).
NIV should NOT be given outside a critical care unit. There is little evidence for this at all in asthma. It needs skill, attention, care, and monitoring. All asthma patients who are put on NIV should have an arterial line. Invasive ventilation may be necessary. There is a choice of sedation and neuromuscular blockade – propofol, (al)fentanyl, xxx-onium. The aim is to minimise patient-ventilator asynchrony. There is a risk of CV collapse on induction. Some people avoid morphine as can cause histamine release (prefer alfentanyl). Prefer vecuronium, rocuronium etc as do not induce histamine release.
Mechanical ventilation is just support, it is not treatment. Progressive dynamic hyperinflation is the major risk. Breath stacking increases thoracic volume —> hypotension. This is a particular risk when patients are manually ventilation in ED – need to have longer I:E ratio – hard to do in pressured environment. Manual bagging should be minimised. Once on a ventilator it is important to watch the monitor in ICU – look at volumes. It may be necessary to disconnect the patient from the ventilator – allow patient to exhale. Manually aid their expiration? 40-50s. Then reconnect. This can be effective in fixing the hypotension / dynamic hyperinflation.
Assessing hyperinflation. Measure plateau pressure – ideally 30cmH20. Measure auto-PEEP – sometimes 10-15cmH20. Interventions to reduce hyperinflation:
- reduce RR (minute volume)
- increase expiratory time, I:E ratio 1:6!
- minimise (external) PEEP
- tolerate hypercapnoea except if concern about (anoxic) brain injury or high ICP
Other therapies? Generally the answer is to get the basics right, wait, and consider ECMO. Heliox is an option – NO (O2 concentration different, have to have special ventilator) but without evidence. Ketamine is suggested as an option, but not used routinely, and also has no good evidence (anecdote, case reports, case series only).
Inhaled anaesthetic agents are again not used routinely, and lack an evidence base (also need specific delivery device etc).
In ECMO oxygenation is determined by the rate of blood flow through device, and configuration of circuit (VV vs AV). CO2 removal is determined by sweep gas flowing through membrane. Allows reduction in ventilator settings and hence ‘lung rest’.
VV ECMO – is ‘respiratory’ support, without CV support. Pump (motor) required. 5L/min can go round VV ECMO circuit but not much more. Returns to venous side of the circulation. If high CO then may not have good systemic oxygenation as returning oxygenated blood mixes with rest of CO. If can provide 2/3 of patients CO through VV ECMO then usually pretty good systemic oxygenation. Small changes in sweep gas can bring big changes in CO2 removal.
AV ECMO = NOvaLung (iLA) – CO2 removal but very little/no oxygenation. Pumpless. Ischaemic complications e.g. need skin graft. Femoral artery to Femoral vein.
See Gaffney et al BMJ article for diagrams of ECMO circuits.
ECMO requires 31FF into RIJV! That is big. There are other VV devices using smaller cannulae. Good for CO2 removal, not v good for oxygenation.
Is there evidence for ECMO in acute severe asthma? There is no RCT for ECMO vs no ECMO for severe asthma. Evidence is all in ARDS.
- Peek, Giles J., et al. “CESAR: conventional ventilatory support vs extracorporeal membrane oxygenation for severe adult respiratory failure.” BMC health services research 6.1 (2006): 163.
The CESAR trial, based at UK Glenfield 2001-2005 showed a benefit to being in a centre that can provide ECMO vs not. However, it suggested that it was not the ECMO that made a difference, rather being in a specialist centre.
- Combes, Alain, et al. “Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome.” New England Journal of Medicine 378.21 (2018): 1965-1975.
ECMO centres in England are in: GSST, Papworth, RBHT, Leicester, S Manchester – these are the commissioned centres. Others may have capacity for ECMO.
Main issue with ECMO is bleeding – give heparin. There is a 5-10% intracranial bleeding in pneumonia. Survival 75% for patients going into ECMO nationally.
Extracorporeal CO2 removal for asthma and severe bronchospasm (ie patients are not ventilated and have Novalung only) ? This is happening and there are good outcomes in asthma on registry data. Requires very careful patient selection. No trial data.
Dr Bastin invited all trainees to come and visit the ICU at Barts! Very welcome.
Biologics for asthma
Paul Pfeffer encouraged anyone interested in asthma research to come and talk to him. There is plenty of research on asthma, and airway disease in London.
Biologics are large molecules, produced in a biological process, difficult to identically replicate and mass produce, and therefore very very expensive.
- Omaluzimab – anti IgE
- Mepoluzimab – anti IL5
- Resluzimab – anti IL5
- Depulimab – anti-IL4/13
- anti-IL33 held up
Lots of biologics are coming which target different parts of the immunological pathway. Most of them work.
Is every eosinophilic asthmatic the same? no. Asthma patients involved in trials are not normal patients. They have to have <10pck yr smoking hx, no bronchiectasis, reversibility on screening day, no co-morbidities, normal ECG, slightly fanatical to engage in all the testing…
Real world data and pragmatic trials are therefore extremely useful.
- Woodcock, Ashley, et al. “The Salford Lung Study protocol: a pragmatic, randomised phase III real-world effectiveness trial in asthma.” BMC pulmonary medicine 15.1 (2015): 160.
- Niven, Robert M., et al. “Impact of omalizumab on treatment of severe allergic asthma in UK clinical practice: a UK multicentre observational study (the APEX II study).” BMJ open 6.8 (2016): e011857.
Niven et al showed that Omaluzimab halves admissions, and exacerbations reduce by 50%. It works in real asthmatics (as well as clinical trial asthmatics).
Biologics are Prescribed through Bluetec. This is the only way to get reimbursed from NHS England, on patient access scheme.
- Hanania, Nicola A., et al. “Exploring the effects of omalizumab in allergic asthma: an analysis of biomarkers in the EXTRA study.” American journal of respiratory and critical care medicine 187.8 (2013): 804-811.
- Pavord, Ian D., et al. “Mepolizumab for severe eosinophilic asthma (DREAM): a multicentre, double-blind, placebo-controlled trial.” The Lancet 380.9842 (2012): 651-659.
Patients may still respond to mepolizumab if they have high eosinophil count but low FeNO (although cut off debatable).
- Lambrecht, Bart N., and Hamida Hammad. “The immunology of asthma.” Nature immunology 16.1 (2015): 45.
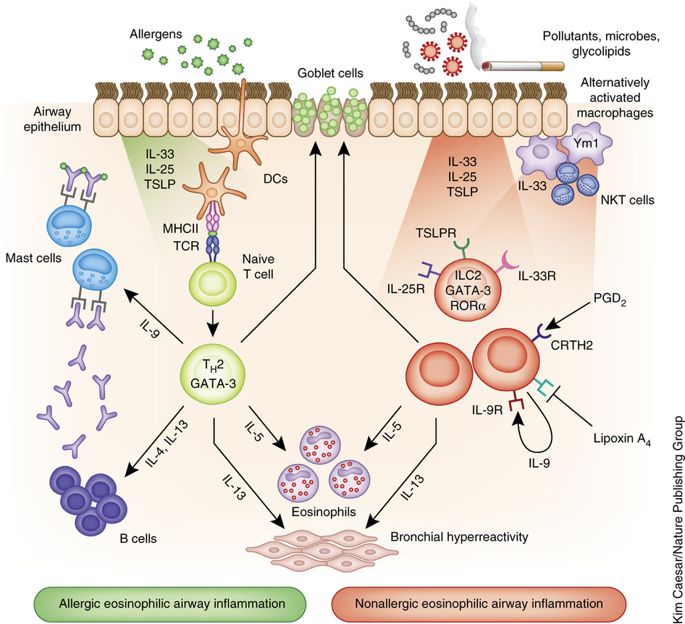
From Lambrecht and Hammad, Nature Immunology
What if a patient is eligible for both anti-IgE and anti-IL5 therapy? If we could phenotype to markers such as IL-33, IL-4, IL-5, IL-13 then we could target treatment appropriately. At present the physician makes a judgement.
- Esquivel, Ann, et al. “Effects of omalizumab on rhinovirus infections, illnesses, and exacerbations of asthma.” American journal of respiratory and critical care medicine 196.8 (2017): 985-992.
In this study outcomes were at 40weeks. It examined the anti-viral actions of omalizumab. Anti-IgE targets dysregulated Th2 immunity higher up and therefore may enhance antiviral actions?
Reslizumab is iv – which means more effort to administer and less appealing to many patients. However, it is effective in those who Mepolizumab has failed.
- Mukherjee, Manali, et al. “Weight-adjusted intravenous reslizumab in severe asthma with inadequate response to fixed-dose subcutaneous mepolizumab.” American journal of respiratory and critical care medicine 197.1 (2018): 38-46
- Varricchi, Gilda, et al. “Reslizumab and eosinophilic asthma: one step closer to precision medicine?.” Frontiers in immunology 8 (2017): 242.
In severe asthma and EGPA, higher dose of mepolizumab has no impact on blood eosinophilia but does have an effect on sputum eosinophilia which is dose dependant. It is safe in asthma but NOT safe in EGPA. Patients may feel better, but have ongoing tissue organ involvement and therefore get a stroke or an arrhythmia. Therefore, do not give Mepolizumab for severe eosinophilic asthma and EGPA.
- Bousquet, Jean, et al. “Care pathways for the selection of a biologic in severe asthma.” (2017): 1701782.
As more biologics become available, MDTs need care pathways to determine which biologic for which patient.

From Bousquet et al 2017
Look out for Dupilumab (anti IL-4/13) and Tezepelumab (anti-TCLP alarmin) on the horizon.

Discussion
No comments yet.