Well done to everyone who made the trek out to Harlow for a day of thromboembolism, CTEPH, ethics, NHS management and asthma. Many thanks to Dr Muhammad Anwar for co-ordinating the day and inviting such great speakers.
Interesting facts about Harlow and the Princess Alexandra Hospital:
- The Princess Alexandra Hospital is a 489 bedded District General Hospital providing a comprehensive range of acute and specialist services to a local population of 258,000 people.
- At the time of the 2011 Census, Harlow had the third-highest proportion of social housing in England, 26.9%, a legacy of the 1947 commitment to re-house blitzed London families after World War II.
- Harlow is the home to a major collection of public sculptures (over 100 in total) by artists such as Auguste Rodin, Henry Moore, Barbara Hepworth, and Ralph Brown. Many of these are owned by the Harlow Art Trust, an organisation set up in 1953 by the lead architect of Harlow Frederick Gibberd. Gibberd had idealist notions of the New Town as a place where people who might not normally have access to art could enjoy great sculptures by great artists on every street corner.

Acute PE: Algorithm, Duration of Therapy, Follow up
Dr Muhammad Anwar, Consultant Chest Physician at Harlow, started the day with a discussion on risk stratification for PE. Options for risk scores include:
- Wells Score
- PERC rule
- PESI – original or simplified
- Troponin I or T
A meta-analysis of the use of troponins concluded “elevated troponin levels identify patients with acute pulmonary embolism at high risk of short-term death and adverse outcome events….Results were consistent for troponin I or T and prospective or retrospective studies.”
- Becattini, Cecilia, Maria Cristina Vedovati, and Giancarlo Agnelli. “Prognostic value of troponins in acute pulmonary embolism a meta-analysis.” circulation116.4 (2007): 427-433.
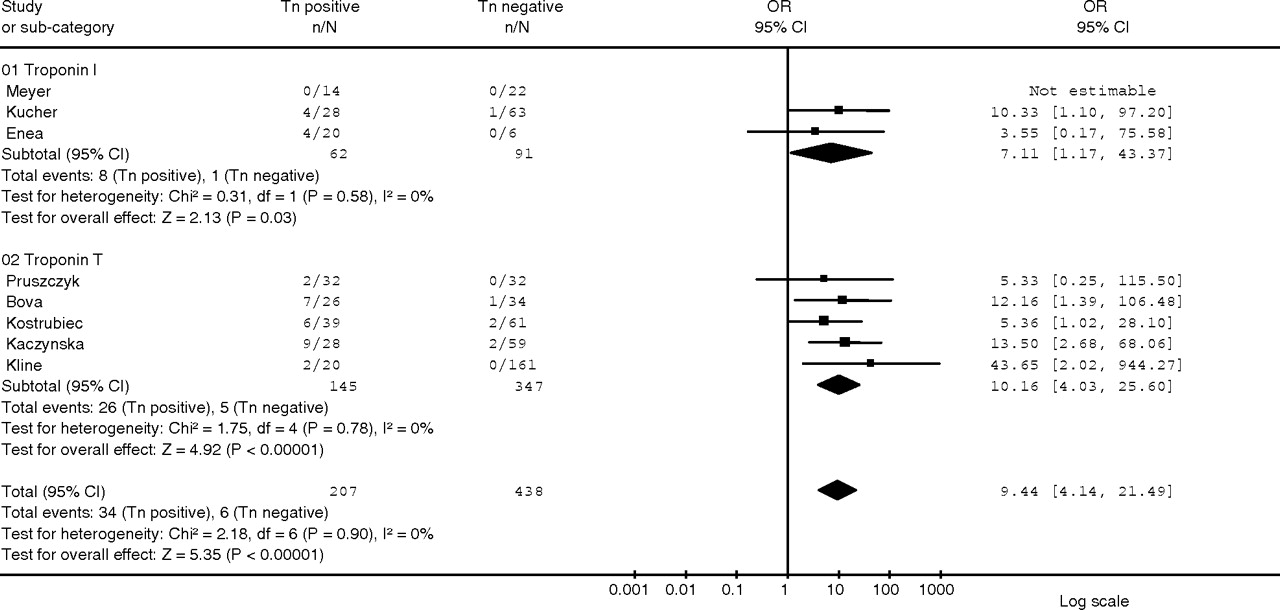
Figure 3 from Becattini et al. OR for death resulting from pulmonary embolism based on elevated or normal serum troponin I and T.
A combination of risk stratification tools has been proposed eg PESI & Troponin.
- Lankeit, Mareike, and Stavros Konstantinides. “Is it time for home treatment of pulmonary embolism?.” European Respiratory Journal 40.3 (2012): 742-749.
Lactate also has some value for short term (ie 7 day) mortality risk. All the above biomarkers have good negative predictive value. They are therefore useful for ambulatory care pathways. A proposal is: PESI 3-5 admit. PESI 1-2 do Troponin and Lactate – if both are negative and there are no additional risk factors then discharge (to ambulatory care with timely review).
We covered some stats to help us think further about risk stratification, particularly for recurrence:
- The risk of recurrence of provoked PE is 5% in 1yr, 15% in 5yr.
- Unprovoked recurrence risk is 10% in 1yr 25% in 5yrs.
- Lifelong anticoagulation recommended for risks >10%. 5-10% is more of a grey area.
A number of risk scores are in use for risk stratification for recurrence of VTE. One is the DASH score is useful for risk assessment for recurrence of VTE.
- Tosetto, A., et al. “Predicting disease recurrence in patients with previous unprovoked venous thromboembolism: a proposed prediction score (DASH).”Journal of Thrombosis and Haemostasis 10.6 (2012): 1019-1025.
- A review: Rodger, Marc, et al. “Unprovoked venous thromboembolism: short term or indefinite anticoagulation? Balancing long-term risk and benefit.” Blood reviews 24.4 (2010): 171-178.
There is an ongoing debate about the utility of screening for malignancy in those who have unprovoked PE. NICE guidelines on this issue suggests a number of investigations including a physical examination, CXR, bloods (FBC, calcium, LFTs) and urinalysis, and consideration of abdo-pelvis CT and mammogram. More evidence has become available since these were produced and they are perhaps in need of updating. A recent study found that the prevalence of occult cancer was low among patients with a first unprovoked venous thromboembolism, and that routine screening with CT of the abdomen and pelvis did not provide a clinically significant benefit.
- Carrier, Marc, et al. “Screening for occult cancer in unprovoked venous thromboembolism.” New England Journal of Medicine 373.8 (2015): 697-704.
The duration of anticoagulation is another area of variation in practice. 3 months is the recommended duration for ‘active treatment’. It is reassuring that the risk of recurrence is the same in this circumstance if anticoagulation is stopped at 3 months, or 6 or 12months. So the decision is 3 months vs indefinite anticoagulation.
- Campbell, I. A., et al. “Anticoagulation for three versus six months in patients with deep vein thrombosis or pulmonary embolism, or both: randomised trial.”BMJ 334.7595 (2007): 674.
- Kearon, Clive, and Elie A. Akl. “Duration of anticoagulant therapy for deep vein thrombosis and pulmonary embolism.” Blood 123.12 (2014): 1794-1801. –> recommended review article, advocating rechecking D-dimer 1/12 after stopping anticoagulation.
ACCP best practice guidelines are available which cover the use of NOACs, and the CHEST website has some useful educational resources on various aspects of anticoagulation.
2014 ESC Guidelines on the diagnosis and management of acute PE come from the Task Force for the Diagnosis and Management of Acute PE of the European Society of Cardiology (ESC) and are endorsed by the ERS.
Radiology in acute PE
Dr Michael Long, Consultant Radiologist in Harlow, discussed who to image, when to image and what modality to choose for acute PE. Guidelines recommend immediately imaging for suspected massive PE, or ASAP with interim anticoagulants for non-massive. There is now the additional problem of incidental PE discovered on cancer staging CTs.
- Cronin, Carmel G., et al. “Prevalence and significance of asymptomatic venous thromboembolic disease found on oncologic staging CT.” American Journal of Roentgenology 189.1 (2007): 162-170.
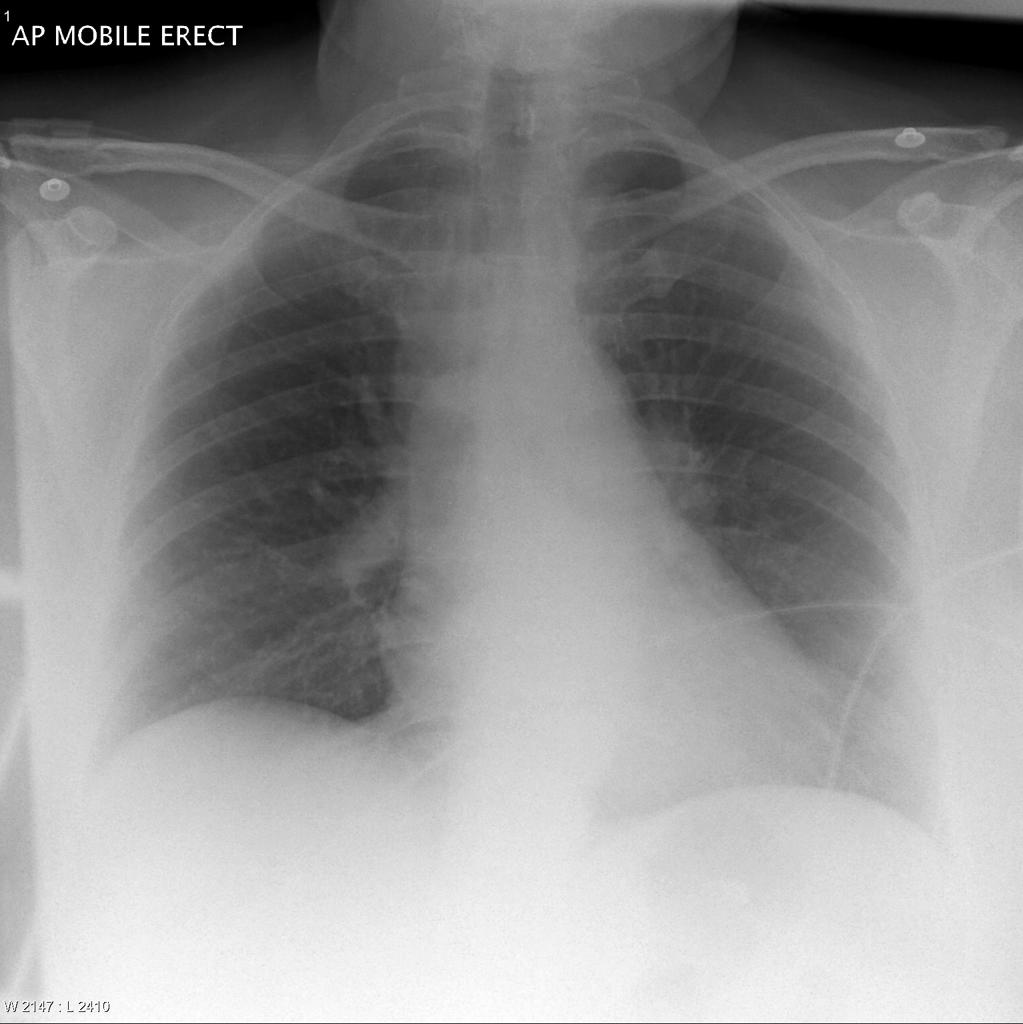
L-sided Westermark. Case courtesy of Jack Ren, Radiopaedia.org. From the case rID: 29131
As we all know CXR is not much use in PE diagnosis. Westermark’s sign, basal atelectasis, and Hampton’s hump are historical signs which are occasionally spotted today, but most often in retrospect. The main use of the CXR is to look for alternative diagnoses. Pleural effusion is also a relatively common sign of PE.
CTPA (spiral CT in arterial phase with a contrast bolus 4ml/sec) is NICE recommended. It has good sensitivity and specificity. It is available 24/7 in all acute hospitals (unlike other possible imaging modalities). Multiplanar reconstructions are very helpful for spotting more subtle PEs. RV > LV diameter on CT is a sign of R heart strain, which SpRs should be able to recognise to aid risk assessment. Image quality is degraded by high BMI (grainy images) and poor contrast (not in phase well so harder to see defect) – 250-300 Hounsfield needed for good diagnosis.
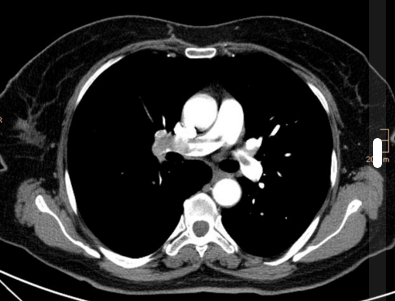
Pulmonary embolism. Case courtesy of Dr Stefan Ludwig, Radiopaedia.org. From the case rID: 13894
VQ and VQ-SPECT are alternatives, using Tc99m. Further discussion of VQ-SPECT including an overview of the evidence, can be found in the notes from the Whittington training day and the Royal Free training day. EANM guidelines for VQ provide guidelines on standardised reporting to support a more binary YES/NO outcome to reporting. MR angiography is problematic due to breathing artefact, and exclusions such as PPM.
PE in pregnancy is challenging due to dose and diagnostic performance. Dose has both deterministic and stochastic effects. For majority of diagnostic medical procedures foetal doses are around 1mGy so risks are low. CTPA and VQ exposure are both in the order of 1 in 1000000 risk of childhood cancer per examination. This is in comparison to a risk of 1 in 500 from natural background radiation. VQ dose is 0.1-0.8mGy and CTPA dose 0.01 – 0.56 mG. More concerning is the effective dose per breast – 0.22-0.28mGy for VQ, 22-50mGy for CTPA. Breast exposure risk is much higher in younger years, and drops after 40yrs. Maternal/foetal radiation favours VQ overall. In addition, physiological changes in pregnancy increase non-diagnostic rate for CPTA. Pregnant women are unlikely to have coexisting lung disease. VQ scans have a high negative predictive value.
Overdiagnosis of PEs is a concern:
- Hoda, Uruj. “Overdiagnosis of pulmonary emboli by CT pulmonary angiograms.” Thorax 69.10 (2014): 925-925.
- Wiener, Renda Soylemez, Lisa M. Schwartz, and Steven Woloshin. “When a test is too good: how CT pulmonary angiograms find pulmonary emboli that do not need to be found.” (2013): f3368.
Acute Sub-Massive PE – Pros Vs Cons Debate
Dr Sarah Clarke and Dr Emma Denneny, ST3 Radiologists from the East of England rotation took us through some of the evidence.
To provide some context we considered a case: a 76 year old man with dyspnoea. Heart rate 68bpm, BP 138/78, RR 24 Sats 97% on 4L. RV dysfunction was seen on ECHO. There were no contraindications to thrombolysis. CTPA showed a LLL PE. We were asked if anyone would thrombolyse. Unsurprisingly no-one said yes! He does not fit the criteria for massive or sub-massive PE from this information.
As we have covered previously, the PEITHO study had a positive result for the composite end point of all cause mortality or haemodynamic collapse within 7 days (p=0.015), but not for the outcome of all cause mortality alone (placebo vs tenecteplase). The study included 1005 patients in a double blind RCT in 76 centres across 13 countries 2007-2012. Follow-up was for 30 days and analysis was on an ITT basis. There were also safety outcomes e.g. bleeding and SAEs. NNT for recurrent PE was 125. There was excess intracranial bleeding in the active treatment group. No guidelines have been published as a result of this trial. The European Society of Cardiology website has up to date guidelines and some useful slides.
The MOPETT trial in 2013 investigated low dose tPA. This trial was not powered for mortality. Instead the primary end points consisted of pulmonary hypertension and the composite end point of pulmonary hypertension and recurrent PE at 28 months. It was a single centre RCT of 121 patients. Patients had moderate PE (not sub-massive), which was defined as 2+ lobar arteries or main artery + signs/symptoms of PE. There were fewer adverse events, and there was a significant immediate reduction in the pulmonary artery pressure that was maintained at 28 months. In the half-dose group less pulmonary HTN. There was no bleeding in either group and no significant difference in mortality.
The TOPCOAT trial took place in 2014, investigating sub-massive PE with a composite outcome including QoL. This was a prospective RCT double-blind multi-centre US trial of 83 patients. The primary composite outcome included: (i) death, circulatory shock, intubation or major bleeding within 5 days or (ii) recurrent PE, poor functional capacity (RV dysfunction with either dyspnea at rest or exercise intolerance) or an SF36 Physical Component Summary score < 30 at 90-day follow-up. The trial was terminated early, apparently because the researcher left! The only significant difference was in one QoL outcome.
In a discussion, we reconsidered the case and thought about what considerations we were taking into account, reflecting on the available evidence. The Cochrane 2015 review called for more evidence. Some people feel that less is more regarding thrombolysis without further evidence. Others risk stratify and lean towards thrombolysing younger patients (due to lower risk of intracranial bleed). We thought about the possibility of catheter directed thrombolysis in the future, but this is not without problems…Current best practice is to carefully weigh up risks and benefits according to current evidence, inform patients fully, and involve more than one Consultant in the decision to thrombolyse sub-massive PE.
Have a look at the resources page for recommendations on useful papers on PE, including a discussion of difficult decisions such as thrombolysis in submassive PE.
Chronic Thromboembolism related Pulmonary Hypertension (CTEPH)
Dr Joanna Pepke-Zaba, Consultant Chest Physician at Papworth reminded us of the types of pulmonary hypertension (PH). PH is a diverse group of diseases affecting the pulmonary circulation (arterial and venous). It is defined as a PAP >25mmHg (RH catheter measure). RV hypertrophy and RH failure are consequences which can lead to syncope, dyspnoea and death.
- PAH – Idiopathic / Inherited / drugs/toxins /associated with e.g. HIV, CTD.
- PH due to LH disease
- PH due to hypoxia
- CTEPH
- Barst, Robyn J., et al. “Updated evidence-based treatment algorithm in pulmonary arterial hypertension.” Journal of the American College of Cardiology 54.1s1 (2009): S78-S84.
- Kim, Nick H., et al. “Chronic thromboembolic pulmonary hypertension.”Journal of the American College of Cardiology 62.25_S (2013).
We focused on CTEPH, which is caused by mechanical obstruction of pulmonary artery branches. It is potentially fatal but potentially curable. The diagnostic criteria for CTEPH requires a RH catheterisation, mismatched VQ defects, and perfusion defects on CT angiogram AFTER 3/12 of anticoagulation. Survival in CTPEH has historically been poor.
- Lewczuk, Jerzy, et al. “Prognostic Factors in Medically Treated Patients With Chronic Pulmonary Embolism.” CHEST Journal 119.3 (2001): 818-823.
The incidence of CTEPH after acute PE varies in different studies dependant on methodology and ranges from 0.5 – 9.1%. Dr Pepke-Zaba suggested the most reliable estimate was 3.8% at 2 years from the Pengo et al study.
- Pengo, Vittorio, et al. “Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism.” New England Journal of Medicine350.22 (2004): 2257-2264.
75% of CTEPH patients give a history of previous PE or DVT, but previous acute PE is not necessary for a diagnosis of CTEPH. More than 1/3 of PH is due to CTEPH. In a national audit the prevalence of CTEPH is 22/million/yr in England (matched for age and sex). There is a Halo effect around PH centres. For example, near Papworth the prevalence is 36/million – likely due to high recognition of disease near a specialist centre.
There is a two compartment model for the pathophysiology of CTEPH. There are occluded vessels (organised thromboembolism) and changes similar to those seen in PAH (secondary response?). In CTEPH it is not a simple thrombus; there is very cellular, fibrosed, reorganised wall plus neo-vascularisation.
- Pepke-Zaba, Joanna, et al. “Chronic thromboembolic pulmonary hypertension (CTEPH) results from an international prospective registry.”Circulation 124.18 (2011): 1973-1981.
Evidence for thrombosis as causative for CTEPH is weak. Classical thrombotic risk factors are not statistically more common. Independent risk factors for CTEPH include: splenectomy, current VTE, infected PPM, malignancy, blood group non-O, APL/lupus anticoagulant, HLA-B*5201, and IBD.
A proposed mechanism is through an ‘inflammatory thrombosis’ with leucocytes and monocytes as key inflammatory markers. CRP and TNF-alpha are elevated in plasma and thrombus tissue.
- Kimura, Hiroshi, et al. “Plasma monocyte chemoattractant protein-1 and pulmonary vascular resistance in chronic thromboembolic pulmonary hypertension.” American Journal of Respiratory and Critical Care Medicine164.2 (2001): 319-324.
It was highlighted that in CTEPH it is not just the small arteries that are abnormal, but also septal veins, bronchial collaterals and bronchopulmonary shunting. Angiogenesis depends on vasa vasorum that derive from systemic bronchial arteries. Collateralisation is more extensive than previously thought. 15-20% of cardiac output is shunted in CTEPH. There is RV-PA coupling – the consequences depend whether the heart is able to cope with the afterload – those with uncoupling develop RH failure.
The diagnostic algorithm of the ESC/ERS guidelines advise that if CTEPH is suspected we should do a VQ scan. If this is positive refer to a PH centre for further investigations. A normal VQ excludes CTEPH. RH catheterisation is the gold standard for diagnosis of PH, in which pressures are measured: RA, RV, main PA, wedge. On CTPA webs, occlusion and pruning are hallmarks. Mosaic attenuation is seen but may be due to small airway disease or perfusion defects. Clinical evaluation includes pulmonary function tests, a 6MWT, ECHO, RH Catheterisation, autoantibody screen, full coagulation screen profile, VQ, HRCT, pulmonary angiogram, and MRI, all of which are discussed at an MDT meeting. Clot location is key, with the key difference being central vs proximal. Proximal clots can be easily accessed by a surgeon.
There is no risk stratification scoring system for surgery which makes patient selection challenging. During pulmonary endarterectomy, surgeons have 20min to clear a lung under deep hypothermic circulatory arrest. We were shown a video and pictures of thrombus removal. An example can be seen online.
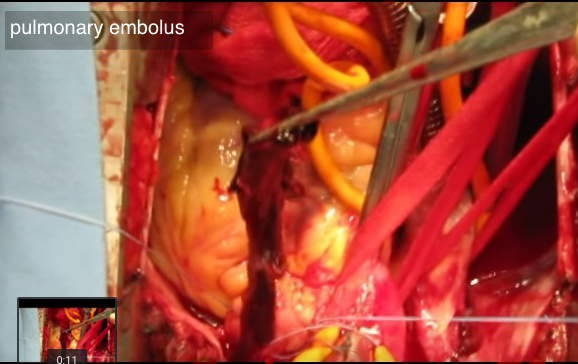
Surgical pulmonary thrombectomy via YouTube
Successful clearance leads to PVR 900dyn/sec/cm5 and improvement in perfusion and RH dynamics. Within 3/12 RH can return to normal size and function.
- Mayer, Eckhard, et al. “Surgical management and outcome of patients with chronic thromboembolic pulmonary hypertension: results from an international prospective registry.” The Journal of thoracic and cardiovascular surgery 141.3 (2011): 702-710.
There have been 1400 operations in Papworth. These have been mostly done for CTEPH but also e.g. chronic thromboembolic disease without PH (if v breathless), sarcoma and vasculitis. The mean age of surgical candidates is 57 +/- 15. Proportions are pretty equal M:F. Usually patients are NYHA III-IV with a mPAP 47mmHg, PVR 795dynes. Good post-op outcomes are a mPAP 26mHg PVR 286 dynes. Longterm survival is related to post-op mPAP. There is 80% survival at 10yrs if mPAP <25mmHg. There is a 2.8% peri-operative mortality. It was up to 20% at the start of the programme. The treatment algorithm is also laid out in the ESC/ESR guidelines. If a patient cannot have a pulmonary endarterectomy they are offered medical treatment (targets 2nd compartment changes). Medical treatment is used for distal disease, residual disease following CTEPH, and those who have too high an operative risk. The usual PAH drugs are used.
- Simonneau, Gerald, et al. “Updated clinical classification of pulmonary hypertension.” Journal of the American College of Cardiology 62.25 (2013): D34-D41.
- Ghofrani, Hossein-Ardeschir, et al. “Riociguat for the treatment of chronic thromboembolic pulmonary hypertension.” New England Journal of Medicine 369.4 (2013): 319-329.
- Simonneau, Gérald, et al. “Riociguat for the treatment of chronic thromboembolic pulmonary hypertension: a long-term extension study (CHEST-2).” European Respiratory Journal 45.5 (2015): 1293-1302.
The CHEST trial was Riociguat vs placebo and showed better 6MWT. There was a trend towards other outcomes. CHEST-2 was an open label trial which had further follow-up. The active group maintained the effects. This is the first licensed drug for inoperable/residual CTEPH. For other treatment options researchers are looking at related fields of coronary and peripheral angioplasty and stents.
- Feinstein, Jeffrey A., et al. “Balloon pulmonary angioplasty for treatment of chronic thromboembolic pulmonary hypertension.” Circulation 103.1 (2001): 10-13.
- Ogo, Takeshi. “Balloon pulmonary angioplasty for inoperable chronic thromboembolic pulmonary hypertension.” Current opinion in pulmonary medicine 21.5 (2015): 425-431.
Research groups in Japan are leading in this area. Numbers are small, with relatively high peri-procedural mortality of 10%. Multiple procedures may be needed to achieve significant haemodynamic effects. RH function improves if a good angioplasty is completed, but the majority of patients still require PAH therapy. The procedure requires precise imaging, high radiation doses, risks of renal toxicity due to contrast, an overnight stay on ITU, and multiple admissions. It is however, a promising technique and was started in Papworth in October 2015. A large MDT is involved. More data is needed…
Ethical Principles in Medicine
Dr Jane Snook, Consultant Geriatric Physician and ethics committee member, Harlow talked us through ethical aspects of every day medicine. She reminded us that there are four core principles of medical ethics: autonomy, beneficence, non-maleficence, and justice.
Case 1: A discussion of a decision not to PEG feed post-stroke. The patient was 82 and had suffered a large L MCA infarct. As a consequence they were bed-bound, unable to communicate, and had made no progress after 2 weeks of treatment which included NG feeding. The MDT felt that a PEG would not be in the patient’s best interests, but family members disagreed. As part of a discussion we highlighted a number of important questions to answer including: whether the patient had an advance statement; whether there was any evidence of progress on treatment; the family’s understanding of the clinical picture including risks and benefits. We were reminded that communication skills and open channels of communication are central. We considered what action could be taken if there continued to be disagreement, including offering a 2nd opinion, providing some time (for a trial of treatment e.g. continue NG feed for further agreed time e.g. 1/52 then review again). It is important to discuss ceilings of care in parallel (ie DNAR discussions). A last resort is to go to court. On the rare occasions that the team believes the family’s decision to not be in the patient’s best interests an IMCA can be invited and there are processes for mediation. If there is a breakdown of trust care can be moved to a different consultant. An ethics committee can provide an independent opinion, particularly as it includes a broad MDT.
Ethical principles relevant to this case: autonomy, non-maleficence. Ethical areas: best interests and end of life care.
Case 2: Involved whether a medical team should disclose that a patient’s daughter had died. The patient had some delirium and the family was adamant that she should not be told. The ward team thought the should be told supportively, and were concerned about the risk of inadvertent disclosure. This case was referred to the ethics committee. In the end she deteriorated and died as an inpatient without knowing. This was clearly complex.
Ethical principles relevant to this case: autonomy. Ethical areas: duty of care.
Case 3: Centred on a young woman with type 1 diabetes who was an inpatient for treatment of DKA, but repeatedly stopped treatment and left the ward to go outside to smoke. A question was raised surrounding the legal and ethical possibilities of stopping treatment in view of the non-compliance. Options discussed included drawing up a contract to facilitate better care. We discussed similar cases that attendees had been involved in. We discussed whether if you don’t believe you will die then do you have capacity?
Ethical principles relevant to this case: autonomy. Ethical areas: consent.
Dr Snook described the work of the Clinical Ethics Committee, an MDT including lay representatives, clergy, social services, palliative care, medical, and surgical professionals. Their role is to support decision-making and patient care. There were 85 committees in 2015 in England. They contribute to local and national guidelines, have an education role, and support clinicians. Cases are the most interesting part of the role. They use an ‘Ethos worksheet’ to facilitate decision making.
We also discussed DNACPR, including the Resus council/BMA guidelines, the GMC 2010 guidelines, and recent cases including Tracey vs Addenbrookes and Winspear vs City Hospitals Sunderland NHS Foundation Trust. We reviewed when DNACPR decisions can and should be made. If a patient is actively dying, is unable to participate in a discussion and it is not possible to contact relatives the medical team can and should make a best interests decision including DNACPR. If the patient is not actively dying then such a decision should wait. If a patient does not have capacity, and has no relatives, an IMCA is required for many decisions. This is particularly important for patients with Learning Disabilities. Patients also have the right to a 2nd opinion about DNACPR decisions.

The UK Clinical Ethics Network site has lots of resources, including case studies, policies, guidelines and details of conferences and seminars. Also, if you’ve never listened to the BBC’s ‘Inside the Ethics Committee‘ you’re missing a treat – real cases discussed by clinicians, ethicists and patients.
Newer Anti-Coagulants for PE (NOACs) – Thrombophilia Screen in PE
Dr Abed Abu Sitta, Consultant Haematologist, Harlow refreshed our memories on the history of warfarin. It was first discovered in 1921 by a Canadian veterinary pathologist. He realised that cattle were ingesting mouldy silage made from sweet clover, and that this was functioning as a potent anticoagulant. As well as its’ infamous use as a rat poison, a number of famous historical figures have been prescribed warfarin, including Eisenhower. Warfarin acts by blocking the action of Vitamin K dependant coagulation factors. Whenever it is prescribed, the risks must be balanced with the benefits. warfarin is particularly challenging due to the risk of bleeding, and the numerous drug interactions.
- Hirsh, Jack, et al. “American Heart Association/American College of Cardiology Foundation guide to warfarin therapy 1.” Journal of the American College of Cardiology 41.9 (2003): 1633-1652.
Reversal of warfarin is with vitamin K (PO/iv) or Beriplex/Octaplex. NOACs have advantages over warfarin due to a more predictable anticoagulation, ease of use (no bridging LMWH), no routine blood tests, good safety profile, and no significnat food/drug interactions.
- Factor Xa inhibitors: Apixaban, Edoxaban, Rivaroxaban
- Thrombin inhibitors: Dabigatran
NOACs are licensed in the UK for: prevention and treatment of VTEs, prevention of CVA in non-valvular AF, but NOT for mechanical heart valves. An RCT of warfarin vs dabigatran in mechanical heart valves REALIGN was stopped early. Valve thromboses require contact factor activation – Factor IX (warfarin affects this but NOACs do not).
Rivaroxaban/Apixaban:
- Apixaban is given BD, and has a shorter half life.
- 66% hepatic, 33% renal excretion. eGFR <15 is an absolute CI. 15-30 reduce dose.
- CYP3AF metabolism plus P-glycoprotein. Potentiated by e.g. azoles, HIV PIs.
Dabigatran
- 80% renal excretion. P-glycoprotein only.
- BD dosing. eGFR <30 is a CI.
- SE: fatigue, headache, N+V, dyspepsia, rash, itching.
Buller, Harry Roger. “Oral rivaroxaban for the treatment of symptomatic venous thromboembolism: a pooled analysis of the EINSTEIN DVT and EINSTEIN PE studies.” Blood (ASH Annual Meeting Abstracts). Vol. 120. 2012. A non-inferiority trial showed a lower risk of recurrence and bleeding compared to enoxaparin. The main advantage is fewer intracranial bleeds – perhaps as it is less able to cross the blood brain barrier. High levels of thromboplastin in the brain may be protective. Doses for prevention of stroke: Rivaroxaban 20mg OD (15mg BD initially post VTE for 3/52)
Apixaban 5mg BD (also needs loading for VTE), Dabigatran 150mg BD.
Prolongation of clotting times on blood tests does not necessarily correlate with bleeding risk. Also ‘normal’ tests does not mean no anticoagulant effect. If bleeding occurs on NOACs can they be reversed? We were advised to use prothrombin complex, N7 or FEIBA, or haemodialysis for dabigatran. Antibodies are becoming available – e.g. for dabigatran. The best advice is to call a haematologist! There are different rules for each of the NOACs pre-surgery – may need 4 days off if poor eGFR and high risk surgery.
Consider thrombophilia testing (for APL) pre starting NOAC as such patients were not included in trials and there has been anecdotal evidence of thrombosis on NOACs. We discussed the possibility of giving NOAC for acute PE on an ambulatory care pathway rather than LMWH. We are not aware of any trusts doing this as yet. Alcohol remains a risk with NOACs as well as warfarin. A clinician recommend warfarin in someone with alcohol dependance as it could be reversed if they have falls, but this is not a straightforward decision. Overall alcohol and anticoagulation is a dangerous combination!
How to work together to improve patient flow and productivity
Richard Hammond, Operations Director, Harlow, gave an excellent talk on NHS management, organisation and funding. The many challenges he faces left us feeling empathetic and depressed!
Some helpful background to the current structure and finding of the NHS can be found at:
- Kings Fund: an alternative guide to the ‘new’ NHS structure in England (CCGs etc)
- The Health Foundation: A report entitled ‘A perfect storm: an impossible climate for NHS providers’ finances?‘ highlights the fact that the funding gap is growing
View the animation at: The Kings Fund
A major driver of NHS management priorities and activity are standards and targets set by central bodies. Examples include: cancer 62 day, 31 day, and 14 day targets; referral to treatment 18wk target; 6wk diagnostics target; 4hr wait in A&E target; and 12hr trolley wait. There are also targets for ambulance turnaround of <60mins. If these targets are not met, the Trust is fined. There are also locally agreed targets with commissioners. Although targets are supposed to drive positive change, the reality can be that organisations work around the targets, seeing them as a distraction, and therefore are unable to focus on what they believe would actually make things better for patients.
The CQC has power over NHS Trusts. It has 5 domains for inspection regarding care: safe, effective, caring, responsive to people’s needs, and well-led. They also provide pathways for whistle-blowing. The CQC carries out planned inspections of health and social care services every 2 years and can also conduct unplanned inspections at any time.
The NHS Standard Contract is published by NHS England. Richard Hammond told us that although there is a draft, the contract is not yet agreed for April 2016 onwards (we are almost in March!). Examples of what might be included in the contract are:
- a local access policy which means that a trust is unable to discharge a patient if they DNA a first appt.
- a requirement for an electronic discharge to reach a patient’s GP within 24hrs ( for inpatient or A&E attendances)
- the duration of medications that will be supplied by the hospital post-discharge
Such changes require investment. All these clauses appear to coming in as part of the 2016/17 contract but have not been agreed yet. In addition to the national contract, there is local contracting which runs from 1st April – 31st March. Commissioning proposals are put in (providers and CCGs), and there is then a debate over activity, during a negotiation period – there is often a mismatch between the CCGs and the providers regarding income assumptions/PBR (payment by results). In reality, the CCG can’t afford to pay for the work actually done by a Trust. The CCGs like block contracts – they pay only for what is agreed, despite the fact that it is known more work will be done than is paid for.
CQUIN – Officially “The CQUIN payment framework enables commissioners to reward excellence, by linking a proportion of English healthcare providers’ income to the achievement of local quality improvement goals.” Some people have called them a CCG cost-avoidance programme! If a community service is set up, this is supposed to stop it coming to the acute Trust. In reality such services often do not prevent the need for the acute trust still doing the work…
SDIPs – Service Development and Improvement Plans are projects which are added to the standard contract. The current hot topic is 7/7 working, which is a planned 2016/17 SDIP. We were asked to define 7 day working – no-one knows what it is!! Trusts lose income if they don’t deliver on an SDIP, even if it’s unachievable!
Best practice tariffs – These are “designed to support commissioners and providers improve the quality and efficiency of care for patients.” In general, money is attached to doing things differently for a specific group, diagnosis or procedure, and the new way earns additional money, while the old way does not (regardless of outcomes). We were given an example of cystoscopy – if it is done as a day case in a day case unit and patient stays 4hrs get £250. If in outpatients get £480. For 2016/7 tariffs are likely to be attached to treatment of heart failure, and parity of mental and physical health, although the specifics are under consultation.
Incentives for 16/17 – commissioners and providers agree the trajectory on four main standards. The provider gets additional funding if they are achieved. This could amount to £2million for Princess Alexandra Harlow if they deliver on all 4 standards! In reality it will be very difficult.
Interestingly, a new national incentive fund was launched just last week: “From April, hospitals and other providers of NHS care will for the first time be funded to improve the support they offer to frontline health staff to stay healthy. They will be able to earn their share of a national incentive fund worth £450m in 2016/17.” The specifics include: access to workplace physio, mental health support, and healthy workplace options (whatever they are); action on junk food and obesity by ensuring that healthy food options are available for their staff and visitors, including those working night shifts; and increasing the uptake of the winter flu vaccine for their staff so as to reduce sickness absence and protect vulnerable patients from infection. The aim is to increase staff vaccination rates from around 50% to nearer to 75%.
In addition to the (difficult to attain) incentives, there are some (easy to attain) fines and penalties:
National:
- Referral To Treatment 52wk incomplete pathway £5k
- Referral To Treatment 18wk breach £300/wk/pt (NB these RTT pathways can no longer be ‘paused’)
- Cancer breach £200 2wk wait £1000
- ED 4hr wait £120 per failure
- 28 day post cancellation failure£0 no payment (ie if you cancel a procedure and don’t rearrange so it happens within 28days you don’t get paid for the procedure, regardless of the reasons for cancellation)
- Not, a fine, but a cap on the activity acute trusts are ‘supposed’ to do. The marginal rate pay on activity above 2009/10 activity is only paid at 30%.
Other:
- Remedial action plans 2% of contract value per month – if fail any 1 of the action plan 2% of the budget is withheld.
- Informational governance breaches, 5% of contract.
Lord Carter’s review has been very influential on how government looks at healthcare funding. He has suggested that large savings can be made by the NHS through efficiencies. The review is based on data from 22 hospitals. He suggests that hospitals must standardise procedures, be more transparent and work more closely with neighbouring NHS trusts
“Lord Carter of Coles’ final report sets out how non-specialist acute trusts can reduce unwarranted variation in productivity and efficiency across every area in the hospital to save the NHS £5 billion each year by 2020 to 2021.”
Lord Carter previously looked at histology services and advised centralisation in order to take advantage of economies of scale. You can judge for yourself how effective that reorganisation bas been for your patients.
Following this insight into the challenges created by existing targets and pay structures, we moved on to think about how clinicians and managers can work together to improve patient flow and productivity, in order to deliver high-quality healthcare. Improving patient flow is essential as there is so little capacity for inpatients, and inpatient care is costly.
Richard shared some of his top priorities for improving patient flow:
- development of high quality safe patient pathways will deliver efficiencies and savings (ie focus on the patient, and the other priorities will follow)
- right person, right place, right time
- avoiding unnecessary acute attendances – options include the acute physician holding the GP referral phone
- turning around those who don’t want/need to be inpatients – best use of alternative pathways eg ambulatory care
- admission avoidance – senior decision makers at (near?) the front door
- keeping LOS to a minimum (manage expectations, set PDD, timely diagnostics)
And for how clinicians can work with managers to enhance productivity:
- Clinical leadership – what does this really mean? Best use of skills and knowledge.
- Input into improving patient pathways (patient flow, Map of Medicine, Assessment units)
- Input into reductions in length of stay (setting PDD at admission, managing expectations, safety-netting)
- Recording of activity undertaken (more accurate coding) – so that trusts get paid appropriately
- Avoidance of penalties/fine (electronic discharge summaries sent out on time are a good first step)
- Support with conditions of the contract – clinicians need to know what these are for a start!
- Understand best practice tariffs and how to achieve them – focus energy on things that matter to patients and clinicians and integrate into ‘normal’ work
One way to quickly make an impact is to work with coders – very different payments given for different codes, which do not always make sense clinically. Knowing how coding is done can help to make sure that notes and discharge summaries are written in a way that ensures the department gets paid appropriately for work done. This can be as simple as using the right terminology (eg influenza-associated pneumonia rather than pneumonia) and including co-morbidities – tweaks like this can lead to significant (and justified) increases in payments. A major tip is never use ? before a diagnosis!
Diagnosis and systematic assessment of severe asthma
Dr Andrew Menzies-Gow, Consultant Chest Physician, from The Brompton Hospital kindly made the trip to Harlow to discuss severe asthma. He highlighted the differing definitions of severe asthma, and the use of multiple terms, which are not always helpful. Severe asthma definitions are based on GINA step 4/5 rather than BTS guidelines.
- Difficult asthma – patient symptomatic despite step IV/V asthma therapy
- Severe asthma -patient has a confirmed diagnosis of asthma and ongoing symptoms despite adherence
- Brittle asthma – not a helpful term. No clear definition.
ERS/ATS guidelines on definition, evaluation and treatment of severe asthma provide good definitions of severe asthma, including the different ways in which it can be uncontrolled.
We considered why severe asthma is important. Often cited figures of use of 50% resources, 15x more likely to use emergency care, 20x more likely to be admitted, are estimates not based on data. To try to assess costs more accurately, modelling was used in a recent Thorax publication. From this, refractory asthma costs £4000/yr/patient. This does not take into account longterm consequences of steroids, or indirect costs. There are an estimated 1.2bn/yr indirect costs – work, looking after children etc. Patients who are on steroids, those with low FEV1 and those who are obese cost more money. In severe asthma there is decreased QoL, side effects from high dose steroids, and increased risk of death. These are difficult conversation to have with a young adult.
- O’Neill, Stephen, et al. “The cost of treating severe refractory asthma in the UK: an economic analysis from the British Thoracic Society Difficult Asthma Registry.” Thorax (2014): thoraxjnl-2013.
In NRAD patients who die do not really die of severe asthma. They die from severe attacks, non-adherence and other causes. In those assessed in a difficult asthma service 60% have severe asthma after a full review. The median age is 40. Patients have the wrong diagnostic label in 10-20%. These include many different diagnoses: pulmonary hypertension, L main bronchus obstruction etc. 30% of patients are non-adherent. Also relatively common are symptoms out of proportion to the degree of obstruction. Dysfunctional breathing is relatively common in asthma. Those who have been in ITU may also have PTSD. Many patients have a combination of these factors, which is why it is so important to treat the whole patient after a systematic assessment.
- Robinson, D. S., et al. “Systematic assessment of difficult-to-treat asthma.”European Respiratory Journal 22.3 (2003): 478-483. (from 102 patients at NHLI/RBH)
Inpatient assessment includes PFTs, histamine challenge, ENT/allergy tests, induced sputum, FeNO, CT, adherence assessment (Prednisolone and cortisol levels), bone densitometry, QoL + psychological assessment, psychologist input, asthma physiotherapist and nurse specialist input. Patients who are overweight also get a sleep study.
- 5% severe asthmatics smoke (compared to 20% mild-moderate) for whom smoking cessation support is essential
- Triggers and allergy – HDM, grass, cats, dogs, aspirin sensitivity (5%?)
- ENT: active rhinitis, sinusitis, nasal polyps, paradoxical movement of the vocal cords
- Later onset non-atopic with nasal polyps – worry about aspirin-sensitivity
- FeNO is useful to track inhaled corticosteroid use
- Dweik, Raed A., et al. “An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications.”American journal of respiratory and critical care medicine (2012).
- Petsky, H. L., et al. “A systematic review and meta-analysis: tailoring asthma treatment on eosinophilic markers (exhaled nitric oxide or sputum eosinophils).” Thorax 67.3 (2012): 199-208.
Clinical health psychologist input is often more useful than psychiatrist assessment. A systematic approach is very important before moving on to expensive therapies lifelong. A specialist systematic approach for severe asthma has been shown to have a number of significant outcomes: unscheduled healthcare utilisation is reduced, patient reported outcomes improve (AQLQ and ACQ). Such outcomes are better than bronchial thermoplastic or many biologics.
- Gibeon, David, et al. “Dedicated severe asthma services improve health-care use and quality of life.” CHEST Journal 148.4 (2015): 870-876.
A survey looked at how difficult asthma is managed. There was a 50% response rate (344).
- Roberts, N. J., D. S. Robinson, and M. R. Partridge. “How is difficult asthma managed?.” European Respiratory Journal 28.5 (2006): 968-973.
Few reported a uniform approach to investigation. The availability of allied healthcare professionals was variable. The 21 consultant respiratory physicians, reporting a special interest in difficult asthma, were significantly more likely to objectively assess compliance, perform skin-prick tests and to utilise a liaison psychiatrist. Many reported difficulty in accessing psychologists, liaison psychiatrists and social workers. Prednisolone and cortisol assays were not available everywhere. This revealed a postcode lottery.
20% of the commissioning budget will be used to commission specialist services. These include: CF, PCD, PH, ILD, and asthma. Referrals to such services can come from primary or secondary care, and patients should fulfil the ERS/ATS definition of severe asthma. There are 10 centres across England, which acts as specialist services and are gatekeepers of high cost drugs and treatments. There are three in London – Brompton, RLH, and Kings.
Current and Future treatment options for severe asthma
Dr Andrew Menzies-Gow also gave us an insight into current and future treatment options for severe asthma, after step V.
Possible steroid-sparing agents include:
- MTX: has very little evidence for efficacy, and significant side effects. It is not a DMARD (only works whilst on it).
- The original paper: Shiner, R. J., et al. “Randomised, double-blind, placebo-controlled trial of methotrexate in steroid-dependent asthma.” The Lancet 336.8708 (1990): 137-140.
- Anti-fungals eg itraconazole: Patients do not have ABPA but are ‘sensitised’. SE profile – monthly LFTs, significant risk of adrenal suppression. Monitor trough levels.
- Denning, David W., et al. “Randomized controlled trial of oral antifungal treatment for severe asthma with fungal sensitization: The Fungal Asthma Sensitization Trial (FAST) study.” American journal of respiratory and critical care medicine 179.1 (2009): 11-18.
- Tiotropium: is advised for step 4. Respimat format. Primary outcome FEV1 – sig better (on top of LABA and ICS), decreased number of exacerbations and increased time to exacerbation. But ACQ and AQLQ not different and no difference in use of rescue medication. TIOSPIR study helped reassure regarding cardiovascular risk.
- Kerstjens, Huib AM, et al. “Tiotropium in asthma poorly controlled with standard combination therapy.” New England Journal of Medicine 367.13 (2012): 1198-1207.
- Bronchial thermoplasty: patients may ask for this after reading the Daily Mail. It was originally developed in dogs. the procedure involves three bronchoscopies 45-60min each under sedation. RLL, LLL, RUL+LUL. There was a sham control in the trial with 1 outcome AQLQ. There was the same improvement in the bronchial thermoplasty and sham procedures. Was there a Haldane effect? Did patients take their inhalers better? In the first 4 months everyone gets worse after bronchial thermoplasty. Then there is a decrease in severe exacerbations and A&E visits. This procedure was approved and is in the NICE 2012 guidance. If patients are referred for this procedure, then the patient has to understand uncertainty around efficacy and long-term safety.
- Castro, Mario, and Gerard Cox. “Asthma outcomes from bronchial thermoplasty in the AIR2 trial.” American journal of respiratory and critical care medicine 184.6 (2011): 743-744.
- Omaluzimab: can be transformational in the right patients. Immunology used to be simple – now it’s not! Blocking IgE or IL5 looked like simple targets. Xolair sc is given every 2-4wks. It binds to free serum IgE which is then removed. It is given to patients with perennial air allergen, IgE 70-700 (and certainly <1500 as above this it is not possible to give sufficient drug to block IgE), on continual (or 4+ courses in a year) oral steroid, and only on a patient access scheme. This is only 10-20% of patients with severe asthma.
- de Groot, Jantina C., Anneke ten Brinke, and Elisabeth HD Bel. “Management of the patient with eosinophilic asthma: a new era begins.”ERJ Open Research 1.1 (2015): 00024-2015.
Risk stratification in asthma needs to move forward. A wish list of biomarkers would include:
- confirmation of diagnosis
- confirmation of adherence to therapies
- risk stratification
- prediction of response to therapies
Asthma is a syndrome. We are now starting to talk about endotypes and phenotypes. For example a Th2 high endotype may be identified due to association with high Th2 cytokines (IL-4/5/13). This is relevant as Th2 type 2 driven inflammation is responsive to steroids.
- Fahy, John V. “Type 2 inflammation in asthma – present in most, absent in many.” Nature Reviews Immunology 15.1 (2015): 57-65.
- Woodruff, Prescott G., et al. “T-helper type 2–driven inflammation defines major subphenotypes of asthma.” American journal of respiratory and critical care medicine 180.5 (2009): 388-395.
- Fajt, Merritt L., and Sally E. Wenzel. “Asthma phenotypes and the use of biologic medications in asthma and allergic disease: the next steps toward personalized care.” Journal of Allergy and Clinical Immunology 135.2 (2015): 299-310.
Precision medicine in asthma will include new biologics. The first wave inhibit IL-5 to target eosinophils: Bendraluzimab – MAb targetting IL-5R on eosinophil itself; Mepoluzimab and Reslizumab – IL-5 blockers, preventing interaction with IL-5R. There are currently no stopping criteria for Mepoluzimab (likely to be licenced in the UK this year) – lifelong therapy at £10,000 a year??
- Ortega, Hector G., et al. “Mepolizumab treatment in patients with severe eosinophilic asthma.” New England Journal of Medicine 371.13 (2014): 1198-1207.
Trials and studies are ongoing with other agents, targeting other parts of the pathways, or other inflammatory mediators. Dupilumab affects IL-4 and IL-13, Tralaknumab IL-13 (currently in phase 2b trials). Will they live up to their promise. Time will tell…
See you all at the next training day at the North Middlesex Hospital on March 31st.

Discussion
No comments yet.